Introduction
The eyes have been provided with a mechanism called accommodation, which results in a change in dioptric power of the eye to see near objects clearly (1, 2). Convergence is a disconjugate movement that allows bifoveal single vision to be maintained at any fixation distance (3). The accommodation and vergence functions of visual reality cause a reduction in visual performance (4). This study aimed to measure the accommodation and vergence measurement after 1 h of mobile gaming.
Subjects and methods
A comparative study was conducted on 50 healthy subjects, in both males and females, with age groups ranging between 18 and 30 years. This study has been approved by the IRB Committee; before the beginning of the study, informed consents were obtained and the procedure was explained clearly; 25 young emmetropic patients and 25 young myopic patients were included. All subjects underwent a comprehensive ophthalmic examination, including vision, subjective/objective refraction, anterior segment examination, accommodation, and vergence parameters, which were assessed before and after playing mobile games for 1 h. The accommodative and vergence facilities were measured using accommodative and vergence flippers. Patients with a history of glaucoma, external eye disease, intraocular or corneal refractive surgery, corneal or intraocular trauma, ocular pathological changes, connective tissue disorders, nystagmus, and other ocular diseases were excluded from this study.

Table 1. Descriptive statistics of age.
Discussion
Accommodation refers to a change in the dioptric power of the eye. Clinically, this is measured either monocularly or binocularly, usually by having the subject fixate on a small target alternately through plus and minus lenses, which are interchanged as soon as the target appears clear. Vergence facility is a simultaneous movement of the pupil of the eyes toward or away from one another during focusing, where movement of one eye is related to the movement of the other. Through analysis, it was concluded that the accommodative facility after playing mobile games has increased significantly than the accommodative facility in both eyes. However, the vergence facility decreased significantly after playing mobile games, and the result was similar to a study done by Uma Mageswari Batumalai et al., who investigated the accommodative response and vergence status by phoria and AC/A ratio method after using virtual reality headset for 30 min and found that there was a significant increase in the accommodative facility and a decrease in the vergence facility after a time of 45 min of virtual reality games (5, 6). Hasebe et al. underwent a study on prolonged exposure of near tasks via virtual reality by headset that may trigger the accommodation. They understood that changes of apparent viewing distance through virtual reality may elicit the level of accommodative response based on apparent stimulus distance(7, 8).
Conclusion
Exposure to virtual reality gaming tends the subjects to focus more and has effect on both accommodation and convergence. Playing for an hour results in lead of accommodation and lag in vergence.
Results
Changes in accommodative facility (OD),(OS),(OU) before and after playing mobile games
In this study, 50 subjects were included, and their accommodative facilities were recorded. This section is intended to test whether the change in accommodative facility (OD),(OS),(OU) before and after playing mobile games is significant or not. For this purpose, a paired samples t-test is applied. The results are shown in Table 2.

Table 2. Accommodative facility (OD),(OS),(OU) before and after playing mobile games.
From Table 2, the t-value of 17.205 (p = 0.000) in OD, the t-value of 17.982 (p = 0.000) in OS, and t-value of 14.983 (p = 0.000) in OU confirm that there is a significant change in the accommodative facility before and after playing mobile games. The comparison is shown graphically in Figure 1.
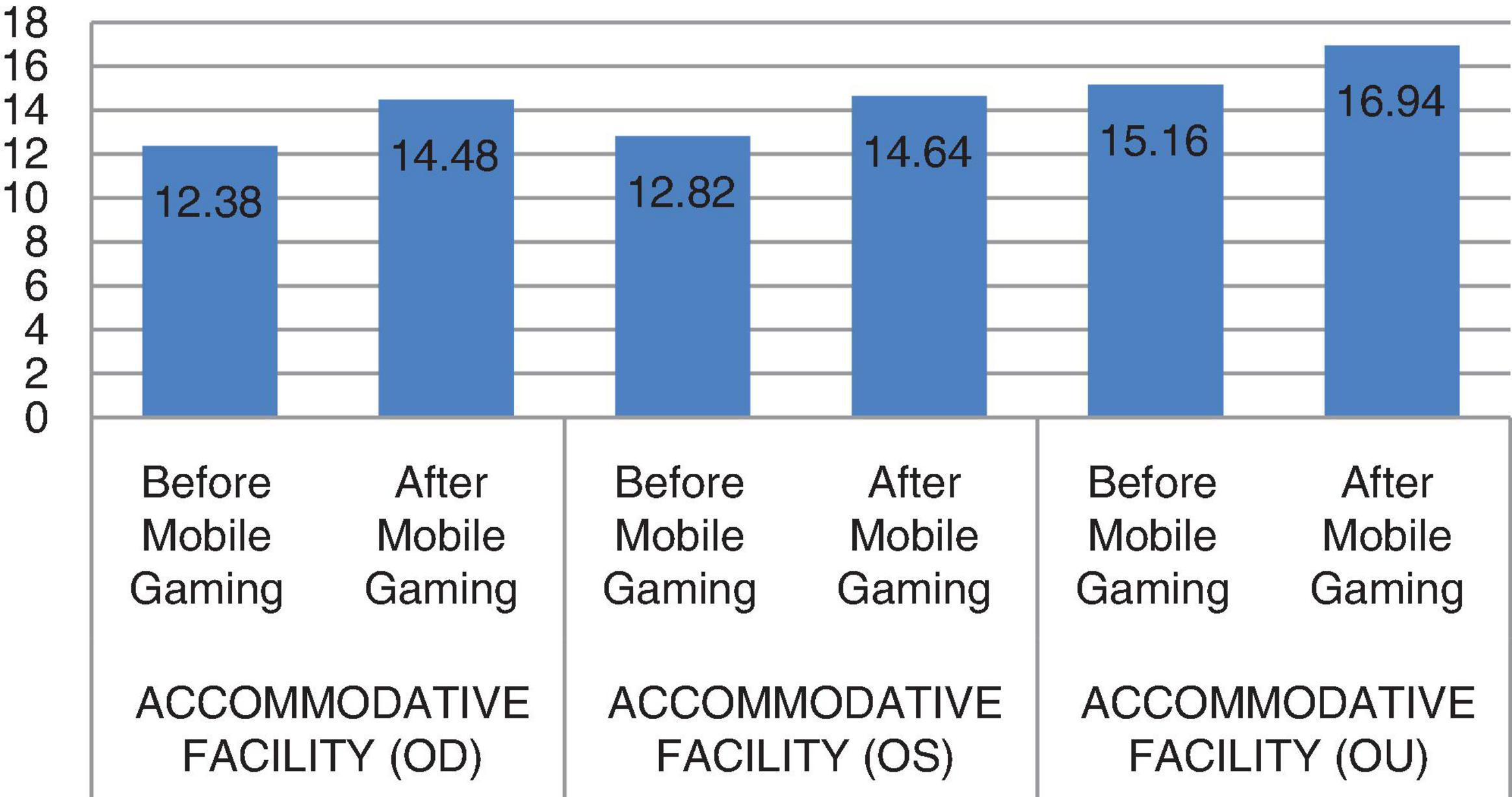
Figure 1. Accommodative facility before and after playing mobile games.
From Table 3, the t-value of 4.451 (p = 0.001) confirms that there is a significant change in the vergence facility before and after playing mobile games. This shows that vergence facility after playing mobile games has decreased significantly than vergence facility before playing mobile games. The comparison is shown graphically in Figure 2.

Table 3. Vergence facility before and after playing mobile games.

Figure 2. Vergence facility before and after playing mobile games.
Author contributions
All authors have contributed equally.
Acknowledgments
The necessary facilities for this work was provided and supported by Saveetha Medical College and Hospital.
References
2. Ciuffreda KJ. Accommodation and its anomalies. In: Charman WN editor. Vision and visual dysfunction. London: MacMillan (1991).
3. Philips R. Physiological optics. In: Hendee WR, Wells PNT editors. The perception of visual information. New York, NY: Springer (1997).
4. Abdul-Kabir M, Kumah D, Koomson N, Afari C. Prevalence of accommodative insufficiency and accommodative infacility among junior high school students in a Ghanaian town. J Sci Technol. (2014) 34:60–4.
5. Borsting E, Rouse M, Deland P, Hovett S, Kimura D, Park M, et al. Association of symptoms and convergence and accommodative insufficiency in school-age children. Optometry. (2003) 74:25–34.
6. Pandian A, Sankaridurg P, Naduvilath T, O’Leary D, Sweeney D, Rose K, et al. Accommodative facility in eyes with and without myopia. Invest Ophthalmol Vis Sci. (2006) 47:4725–31.
7. Peter M, Allen W, Charman N, Radhakrishnan H. Changes in dynamics of accommodation after accommodative facility training in myopes and emmetropes. Vision Res. (2010) 50:947–55.