Introduction
Microblepharon an atypical presentation characterized by shortening of the anterior lamella of the upper eyelid. It was first stated by Cornaz in 1848 (1), and later Fuchs described its features in 1885 (2). It is associated with multiple congenital anomalies such as microphthalmos, lid coloboma, absence of puncta, and tetrastichiasis with anomalies of the limbs, genitals, face, and skull (3–7). Isolated microblepharon case without systemic and ocular abnormalities has also been reported.
Case report
A 9-month-old child with Down’s syndrome presented with complaints of inability to close eyelids since birth, photophobia, whitish discoloration of corneas, and watery discharge from both eyes. Although no karyotyping was done, Down’s syndrome was diagnosed based on facial phenotypic features. Clinical ocular examination revealed bilateral upper eyelid microblepharon associated with ectropion and significant lagophthalmos with exposure of keratopathy in both eyes, which was more in the right eye than in the left eye (Figure 1). The patient was prescribed topical antibiotics and frequent lubrication and referred to the pediatrician for thorough systemic evaluation. The pediatric consultation revealed no systemic anomaly, and we scheduled for urgent surgical modification of the bilateral upper lid microblepharon with ectropion correction to attain eyelid closure. A full-thickness skin grafting of bilateral upper eyelid was done with a graft from the retroauricular donor area (Figure 2). Ectropion was almost corrected following skin graft, although lateral lid tightening was done by lateral tarsal strip (LTS) procedure. Postoperatively, there was minimal lagophthalmos, and keratopathy was resolved (Figure 3).
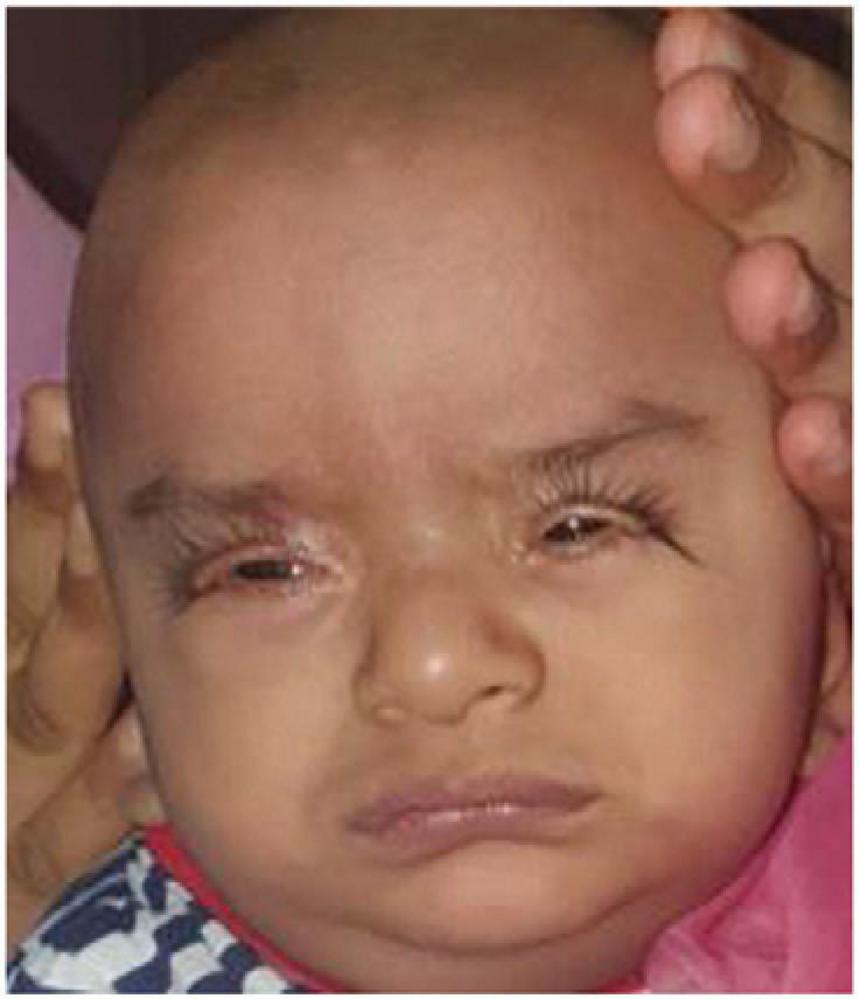
Figure 1. A 9-year-old baby with Down’s syndrome presented bilateral upper eyelid microblepharon and ectropion associated with severe photophobia

Figure 2. Correction of microblepharon with a full-thickness skin graft

Figure 3. Three months postoperatively after correction of microblepharon (no photophobia due to resolution of keratopathy).
Discussion
Microblepharon is a rare hereditary anomaly categorized by vertical shortening of anterior lamellae of the eyelids (1). Fuchs defined vertical eyelid height (VEH) as the space between the upper eyelid margin and the center of the eyebrow with the eyes closed and vertical eyelid length (VEL) as the distance from the center of the eyelid margin to the center of the eyebrow when the eyelid is maximally stretched. Typically, the ratio of VEH and VEL is more than 1.5; when it is less than 1.5, microblepharon is suspected. In our case, both VEH and VEL were 6 mm, and therefore the ratio was 1.
Microblepharon is a bilateral condition, but it may occur unilaterally on rare occasions (8). Microblepharon presents various clinical signs, such as mild lagophthalmos with watering of eyes, photophobia, ectropion, and severe lagophthalmos, causing inadequate closure of the eyelids and corneal exposure-related problems. In some literature, microblepharon has been reported in a stillbirth (9). There are also reports in children with ectropion and bilateral aphakic-microphthalmos (10). Merriem et al. (11) have described microblepharon to be associated with multiple congenital anomalies. It has also been reported with chromosomal abnormalities like trisomy 21 and trisomy 12p (12). Down’s syndrome includes ocular deformities like myopia, keratoconus, nystagmus, epiblepharon, brush fields spots, hypertelorism, epicanthus, convergent strabismus, cataract, blepharoconjunctivitis with the epicanthal folds, and the characteristic mongoloid slant to the eyelid fissures (13). In our case, no other ocular comorbidities were noted, except mongoloid slant to the eyelid fissures on examination under anesthesia.
If we consider embryogenesis, the lower eyelids develop from the maxillary processes and the upper lids from the frontonasal prominence (14). By day 45, both the upper lid and lower lid folds begin to develop, grow toward each other, and fuse at around the third month and again separate at around the sixth month. The mesenchyme of the lid fold is derived from the neural crest, and its deficiency can cause microblepharon.
The management of the microblepharon depends on its severity. In the case of mild lagophthalmos, the cornea is well protected from being treated with lubricating eye drops and ointment. In severe lagophthalmos, cornea exposure leads to keratitis and may need surgical intervention to preserve vision. The surgical procedures mainly involve eyelid reconstruction with free, full-thickness skin grafts or pedicle flaps. In our case, we did the upper lid reconstruction with full-thickness skin grafts. Postoperatively, there was negligible lagophthalmos. Subsequently, the keratopathy healed, the left cornea is clear, and only a mild scar on the right cornea. Our observation is urgent surgical intervention needed to attain good corneal coverage and preserve sight. The child is on follow-up and may require additional visual rehabilitation.
Statement of ethics: The patient’s parents gave knowledgeable consent to publish this case report (text and photographs). The institute’s committee approved the study protocol on human research. The study involved no animal research.
Disclosure statement: This study did not draw definite sponsorship or funding. There are no conflicts of interest.
References
1. Jordan D, Hwang I, Pashby R. Microblepharon: a case report. Ophthalmic Surg Lasers. (2000) 31:502–5.
2. Fuchs E, et al. Zur physiologie und pathologie des lidschlusses. Albrecht Von Graefes Arch Klin Exp Ophthalmol. (1885) 31:97–120.
3. Urmetzer J, et al. Ein fall von abnormerkuerze der lider. Klin Monatsbl Augenheilkd. (1914) 53:240.
4. Von Herrenshwand F, et al. Ueber ectropium conjunctivae palpebral congenitum. Klin Monatsbl Augenheilkd. (1916) 56:477–83.
5. Landau J. A case of congenital vertical shortness of the lids combined with tetrastichiasis. Br J Ophthalmol. (1947) 31:219–23.
6. Waardenburg PJ. A twin monster with remarkable ocular anomalies. Ophthalmologica. (1954) 128:268–70.
7. Gallenga C, et al. Contributoallo studio di alcune deformita conigeniitedelle palpebre. G Accad Med Tor 40: 625–728. Int Ophthalmol. 123.
8. Bernardini F, Kersten R, de Conciliis C, Devoto M. Unilateral microblepharon. Ophthalmic Plast ReconstrSurg. (2004) 20:467–9.
10. Klauss V, Mnyalla N, Dechant W, et al. Beid seitiges kongenitales mikroblepharon mit ektropium und microphthalmus. Klin Monatsbl Augenheilkd. (1981) 179:366–7.
11. Merriam J, Stalnecker M, Merriam G. Reconstruction of the lids of a child with microblepharon and multiple congenital anomalies. Trans Am Ophthalmol Soc. (1988) 86:55–93.
12. Tekin M, Jackson-Cook C, Pandya A. De novo inverted tandem duplication of the short arm of chromosome 12 in a patient with microblepharon. Am J Med Genet. (2001) 104:42–6.
13. Gilbert H, Smith R, Barlow M, Mohr D. Congenital upper eyelid eversion and Down’s syndrome. Am J Ophthalmol. (1973) 75:469–72.