Introduction
Preeclampsia is a hypertensive disorder of pregnancy that significantly affects maternal and fetal health. It is characterized by high blood pressure and signs of organ damage, often manifesting after 20 weeks of gestation (1). Hypertensive disorders in pregnancy contribute to approximately 10% of maternal deaths globally, with preeclampsia and eclampsia being the primary causes (2). In developing countries, including Zimbabwe, preeclampsia remains a leading cause of maternal and neonatal morbidity and mortality. In Zimbabwe, preeclampsia and its complications are a significant public health issue, particularly in rural areas where access to prenatal care and health facilities is limited (3).
Most maternal health facilities in Zimbabwe, including Victoria Chitepo Provincial Hospital (VCPH), often face shortages of resources and inadequate healthcare infrastructure, which can impede the identification and management of women with preeclampsia (4). Despite the significant impact of preeclampsia on maternal and fetal health, there remains a lack of comprehensive data on its prevalence in various healthcare settings across Zimbabwe.
Fetal outcomes are equally concerning, as preeclampsia is associated with a higher risk of preterm birth, low birth weight, and stillbirth (5). The relationship between maternal and fetal outcomes necessitates a holistic approach toward managing pregnant women with preeclampsia to mitigate these risks.
Sub-Saharan Africa has the highest maternal mortality ratio at 500 per 100,000 live births (5). In Zimbabwe, preeclampsia and eclampsia are the third leading causes of death after human immunodeficiency viruses (AIDS)-defining conditions and postpartum hemorrhage. Hypertensive disorders also indirectly contribute to maternal deaths by being a common risk associated with postpartum hemorrhage. Preeclampsia is a leading cause of maternal morbidity and mortality in Zimbabwe (6). According to the Zimbabwe National Health Profile (2020), hypertensive disorders contribute significantly to maternal deaths, with preeclampsia accounting for a considerable proportion. At VCPH there has been a noticeable rise in hypertensive-related complications during pregnancy, including preeclampsia and its severe manifestations such as eclampsia. These conditions result in preterm births, low birth weight infants, and stillbirths. However, there is limited data available to assess the prevalence of preeclampsia specifically at VCPH, as well as its fetomaternal outcomes. This lack of data hinders the ability to implement targeted interventions and may contribute to the continued high rates of maternal and neonatal mortality.
The prevalence of preeclampsia can vary greatly by region and healthcare setting, highlighting the necessity of localized studies to determine specific risk factors and outcomes in populations.
There is a need to generate reliable data on the prevalence of preeclampsia at VCPH and assess its impact on maternal and fetal health. Hence, the main objective of this is to assess the maternal and fetal outcomes associated with preeclampsia among pregnant women attending VCPH.
Methodology
Research design
The proposed research adopted an analytical cross-sectional design. In this type of research, data were collected from, the hospital medical records, laboratory results records, and patient charts. The prevalence of preeclampsia and related fetomaternal outcomes was assessed at a specific point of time from January 2023 to December 2024.
Study population
The study population comprised all pregnant women, whether diagnosed with preeclampsia or not, who were admitted to VCPH, located in Mutare, Zimbabwe, from. January 2023–December 2024. This facility serves a diverse population, catering specifically to low- to middle-income women from surrounding communities who require maternal healthcare services.
Inclusion and exclusion criteria
We included pregnant women aged 18 years and above who were admitted to VCPH over the selected time frame. The age criterion was set at 18 years and above to align with the World Health Organization’s classification of adulthood, providing consistency in the study’s demographic focus.
Sampling procedure and sample size
The simple random sampling was used yielding a sample size of 3,484 pregnant women admitted to VCPH from January 2023 to December 2024 who met the inclusion criteria. The sampling procedure involved systematically identifying all eligible participants based on hospital records who meet the inclusion criteria.
Study setting
Data were collected from the VCPH, a major health facility in Mutare, which has the capacity and resources for managing high-risk obstetric cases. The maternity ward is optimized for maternal health, integrating various specialists to handle complications arising during labor and delivery.
Bias
To deal with bias and confounding variables, we strictly adhere to the inclusion criteria, and simple random sampling was applied to sample our study population.
Data analysis
Descriptive statistics were utilized to determine the prevalence of preeclampsia, and chi-square was applied to explore relationships between preeclampsia and described fetomaternal outcomes. Reliability and validity of the data were ensured through careful management of the database, including checks for consistency and accuracy.
Ethical considerations
Ethical clearance to conduct the study was sought from the Africa University Research Ethics Committee (AUREC). Ethical approval number AUREC 3857/25 Permission to review clinical records was obtained from the Laboratory Chief Scientist at VCPH.
Results
Socio-demographic characteristics of the study population
A total of 3,484 participated in the study. Age and residency, whether from rural or urban, contributed significantly to the prevalence of preeclampsia among women. Women from rural areas were the most preeclamptic, with 69.2% (129) compared to the 30.8% (59) preeclamptic pregnancies from urban areas. The most dominant age group was 30–35, with 26.1 and 9.0% for preeclamptic deliveries for rural and urban areas, respectively. The least preeclamptic pregnancies were from the age group 42+ with a total of 10.1% (19) deliveries (Table 1).
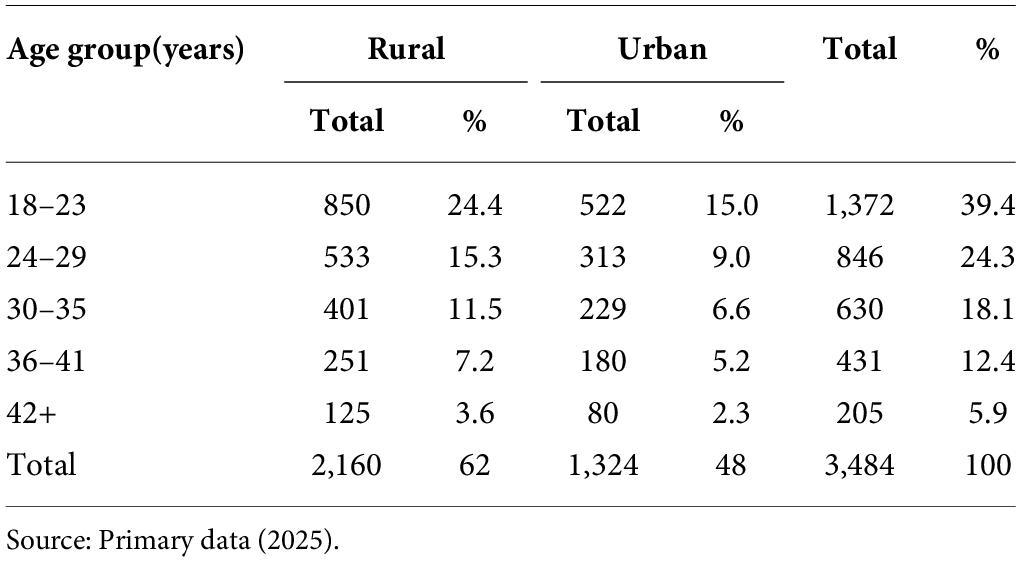
Table 1. Socio-demographic characteristics of the study population (N = 3484).
Prevalence of preeclampsia among pregnant women admitted to VCPH
Of the total number of women who were under the study of 3,484 who participated in the study, those who were from the rural areas had the most preeclampsia pregnancies at 3.70% (129). Those from the urban areas had the least preeclamptic cases, with 59 cases constituting 1.67%. However, the age group of 30–35 had the most preeclamptic cases than any other age group, with 1.89% (66). The least age group with preeclamptic cases was 42+, which has 19 cases constituting 0.54%. The table however deduced that the prevalence of preeclamptic pregnancy cases was 5.37%, which constituted 188 of the whole study population of 3,484 (Table 2).

Table 2. Stratified prevalence of preeclampsia by age group and residency (N = 188).
Maternal outcomes associated with preeclampsia among pregnant women
This section presented the complications that were found (Table 3).

Table 3. Maternal outcomes associated with preeclampsia among women (N = 188).
The results of chi-square for maternal outcomes due to preeclampsia are shown in Table 4.

Table 4. Chi-square test of maternal outcomes associated with preeclampsia (N = 3484).
The data showed there were association between the age groups 18–23, 30–35, 36–41, and >42 years with preeclampsia. Focusing on the maternal outcomes, hemorrhage had the most impact on maternal outcomes associated with preeclamptic pregnancies (Table 4).
Foetal outcomes in preeclampsia
The results obtained by this study showed that of the 188 deliveries in 2023 and 2024 associated with preeclampsia.
The data (Table 5) showed that 45.7% (84) who had preeclamptic pregnancies developed fetal outcomes. Those that did not develop fetal outcomes were 54.3% (104 cases). The highest number of cases was found in preterm births, a total of 27 cases (38.4%). However, it was noted that across all the fetal outcomes, there was a reduction in cases as the age increases; hence, for all fetal outcomes, the most cases were found in the 18–23 age group, with the least cases found in the 42+ age group.

Table 5. Fetal outcomes in preeclampsia pregnancies (N = 188).
Neonatal mortality, stillbirth, and preterm were not associated with preeclampsia. However, the age groups with the highest fetal outcomes were found to be 18–23 and 30–35, as well as the low birth weight (p < 0.05) (Table 6).
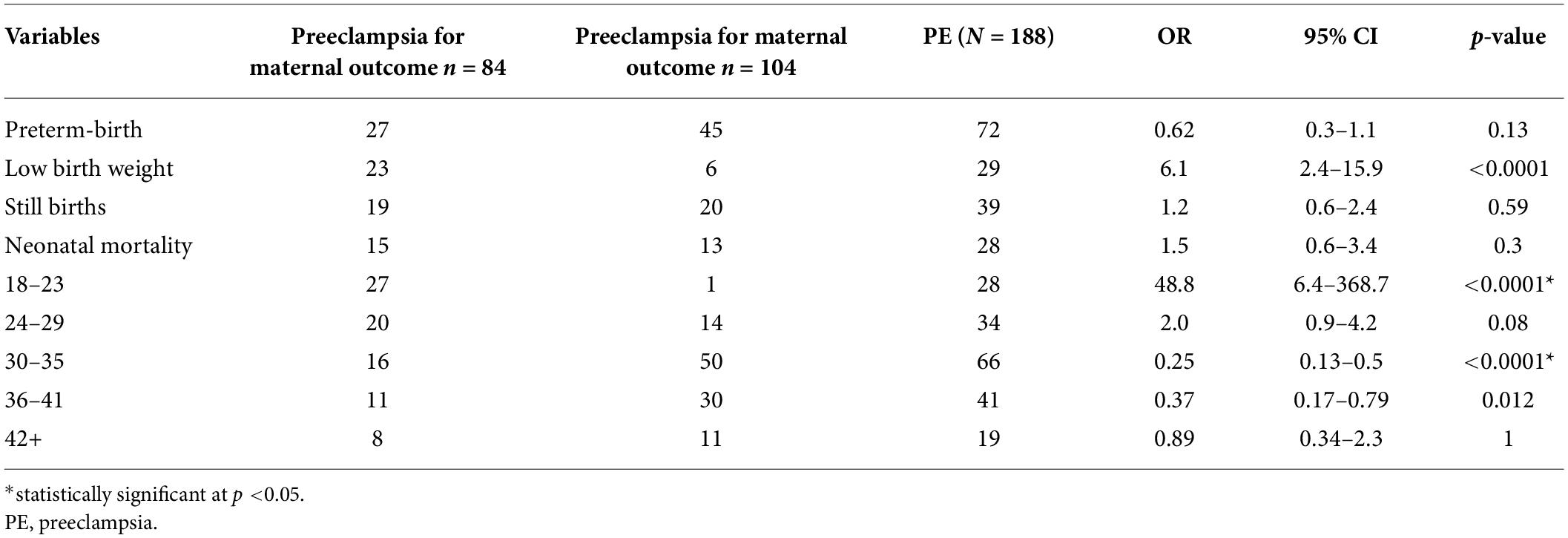
Table 6. Chi-squared of fetal outcomes in preeclampsia (N = 188).
Clinical factors associated with preeclampsia
The data showed that obesity, gestational hypertension, chronic hypertension, diabetes mellitus, and renal diseases were considered to provide information for the demographic and clinical factors associated with preeclampsia among pregnant women attending VCPH (Table 7).

Table 7. Clinical factors associated with preeclampsia among pregnant women (N = 188).
The data above (Table 7) showed that out of 188 preeclamptic women, 142 were affected by the clinical factors. This constituted a 75.5% chance for preeclamptic women to have the complications stated. The data above showed that the most prevalent clinical factor was chronic hypertension, with 21.3% constituting 40 cases in preeclamptic women. The least prevalent factor was gestational hypertension, with 9.6% constituting 18 cases. However, renal diseases can potentially affect individuals in various age groups. However, in the context of preeclampsia pregnancies, renal diseases may have a more significant impact on older age groups. The order from highest to lowest risk of renal diseases affecting age groups in preeclampsia pregnancies. The chi-squared was tested to assess the association between the clinical factors and preeclamptic cases (Table 8), which showed that the clinical factors that have the most impact on preeclamptic pregnancies are mainly chronic hypertension, gestational hypertension, and age ranges 18–23, 24–29, 30–35, and 42+ with p-value < 0.05.

Table 8. Chi-square test on clinical factors associated with preeclampsia (N = 188).
Discussion
Preeclampsia affects approximately 2–8% of pregnancies globally, making it a common and serious pregnancy complication that can lead to adverse maternal and fetal outcomes if not managed properly. The present study has shown that there is a higher prevalence of preeclampsia among women living in rural areas compared to those in urban areas. This was similar to a study conducted in Ghana, where women in rural areas are at a higher risk for preeclampsia pregnancies (7) compared to urban. Similarly, a study in Thailand also reported a higher prevalence of preeclampsia among women in rural areas (8). However, it is important to note that not all studies have found a higher risk of preeclampsia in rural areas. Gong et al. (9) argued that the association between rural residence and preeclampsia may be confounded by factors such as race, socioeconomic status, and access to healthcare. However, it is important to note that this critique has been largely overshadowed by the numerous studies and evidence supporting the higher prevalence of preeclampsia in rural areas. The prevalence of preeclampsia among women admitted at VCPH was found to be 5.37%. Several studies have reported similar prevalence rates of preeclampsia in different settings. For example, a study in Nigeria found a prevalence rate of 5.8% among pregnant women attending antenatal clinics (10). Similarly, a study done in Brazil reported a prevalence rate of 4.6% among pregnant women in a tertiary care hospital (11). These studies support our study findings and highlight the consistent burden of preeclampsia in different countries and healthcare settings.
The prevalence rate of preeclampsia found in our study is significant in the context of global preeclampsia prevalence, as it falls within the range of reported prevalence rates worldwide, at the opposite end of another study conducted in Zimbabwe at Mpilo Central Hospital. The incidence of preeclampsia was 1.3% (12), which is below the global prevalence; this discrepancy could be attributed to the difference in research setting.
The maternal outcomes mainly associated with preeclampsia in this study are mainly chronic hypertension, gestational hypertension, hemorrhage, and the age groups 18–23, 24–29, 30–35, and 42 years. This corroborate with previous study whereby hemorrhage, pulmonary edema, acute renal failure, or Disseminated Intravascular Coagulation (DIC) could occur due to long-term effects of cardiovascular disease (13, 14), as well as with another study conducted in Zimbabwe where hypertensive disorders of pregnancies were significantly associated with preeclampsia (15). With respect to the age group, advanced maternal age is associated with age-related changes in vascular health, such as reduced flexibility of blood vessels and impaired endothelial function, which are factors that can predispose women to the development of preeclampsia (16). Younger women may face unique risk factors that increase their vulnerability to maternal mortality, such as inadequate prenatal care, higher prevalence of unplanned pregnancies, limited access to healthcare services, and socioeconomic challenges. Maternal complications of severe preeclampsia/eclampsia can be serious, leading to maternal, fetal, and neonatal morbidity and mortality. These include Hemolysis, Elevated Liver enzymes, and Low Platelet count (HELLP) syndrome, disseminated intravascular coagulopathy, and acute renal failure (17); however, with regard to renal disease, our finding did not observe any statistical significance on this risk factor.
With regard to fetal outcomes in this study, neonatal mortality, stillbirth, and preterm were not associated with preeclampsia. This corroborate with a study by Hidalgo-Lopezosa et al. (2019), which found that the percentage of neonatal mortality in preeclamptic pregnancies was only 4.8%, indicating a relatively low risk of neonatal death in these cases (18).
Low birth weight as fetal outcome was significantly associated with preeclampsia in this study. This is in agreement with another study conducted in Zimbabwe (12), where the most common fetal/neonatal complications were stillbirths, prematurity, and very low/low birth weight; however, our study did not find any statistical significance on stillbirths or prematurity. This could be likely due to our moderate sample size.
However, it was noted that across all the fetal outcomes, the most significant fetal outcomes are found in the 18–23 and 30–35 age groups. Younger pregnant women, particularly adolescents, may not have fully developed reproductive systems and may not be fully physically mature, which can increase the risk of complications during pregnancy and childbirth (19). Younger pregnant women may be less likely to seek prenatal care or may delay seeking medical attention, which can result in undetected or untreated pregnancy complications that increase the risk of adverse fetal outcomes (20).
The findings from our study were critical in Zimbabwe, where few literatures exists that sheds light on the profound serious impacts that severe preeclampsia has on maternal, fetal, and health. It is of key importance to provide universal antenatal care to pregnant women as a preventive strategy. To the global policy makers, this study gives insight into helping tackle one of the major contributors to global maternal and neonatal morbidity and mortality. However, our study has some limitation, such as that it is localized; hence, it could be interesting to extend it to a wider population across the country and incorporate more variables of studies as well as expend the sample size.
Conclusion
The prevalence of preeclampsia amongst women was 5.37% and was quite high when compared to similar studies conducted in other Zimbabwe provinces. Maternal outcomes associated with preeclampsia were postpartum hemorrhage and lower birth weight, which were the most frequent in fetomaternal outcomes for women affected with preeclampsia. Chronic hypertension and gestational hypertension are the most fatal clinical factors for pregnant women to have preeclampsia. The age groups with the highest fetal outcomes were found to be 18–23 and 30–35. The findings from this study are of vital importance in the prediction of adverse outcomes in preeclampsia in Zimbabwe due to the higher incidence of preeclampsia reported in the country. In order to alleviate the burdens on maternal, fetal, and neonatal health, governments should focus on educating women about the dangers of preeclampsia/eclampsia so that they present early to hospitals. This would help prevent complications.
Author contributions
TC: Conceptualization, Data curation, Writing – original draft. MTMS: Data analysis, Writing – review and editing. TC and MTMS: Project design. All authors agree to be accountable for the content of the work.
Funding
This work did not receive any funding.
Acknowledgments
The authors wish to thank Africa University and VCPH for providing data and facilitating this research.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Banala C, Moreno S, Cruz Y, Boelig RC, Saccone G, Berghella V, et al. Impact of the ACOG guideline regarding low-dose aspirin for prevention of superimposed preeclampsia in women with chronic hypertension. Am J Obstet Gynecol. (2020) 223(3): 419.e1–e16.
2. Ragasudha C, Madhavi AP, Sharon PS, Priya SS, Shehnaz S. A study of maternal deaths from preeclampsia and eclampsia in a tertiary care centre. IAIM. (2018) 5(1):6–10.
3. Robbins T, Musiyiwa M, Gidiri MF, Mambo V, Hill C, Sandall J, et al. Developing shared understanding of pre-eclampsia in Haiti and Zimbabwe using theory of change. PLoS Glob Pub Health. (2022) 2(12):e0001352.
4. Manna B, Mandal S, Ghosh P, Pal DK. An observational study on posterior reversible encephalopathy syndrome in severe preeclampsia and eclampsia. Int J Acad Med Pharm. (2023) 5(4):194–9.
5. Ray JG, Abdulaziz KE, Berger H. Aspirin use for preeclampsia prevention among women with prepregnancy diabetes, obesity, and hypertension. JAMA. (2022) 327(4):388–90.
6. Ngwenya S. Postpartum hemorrhage: incidence, risk factors, and outcomes in a low-resource setting. Int J Women’s Health. (2016) 8:647–50.
7. Adu-Bonsaffoh K, Obed SA, Seffah JD. Maternal outcomes of hypertensive disorders in pregnancy at Korle Bu Teaching Hospital, Ghana. Int J Gynecol Obstet. (2014) 127(3):238–42.
8. Boriboonhirunsarn D, Pradyachaipimol A, Viriyapak B. Incidence of superimposed preeclampsia among pregnant Asian women with chronic hypertension. Hypertens Pregnancy. (2017) 36(2):226–31.
9. Gong S, Sovio U, Aye ILMH, Gaccioli F, Dopierala J, Johnson MD, et al. Placental polyamine metabolism differs by fetal sex, fetal growth restriction, and preeclampsia. JCI Insight. (2018) 3(13):e120723.
10. Bokslag A, van Weissenbruch M, Mol BW, de Groot CJM. Preeclampsia; short and long-term consequences for mother and neonate. Early Hum Dev. (2016) 102:47–50.
11. Mazarico E, Peguero A, Camprubí M, Rovira C, Roig MDG, Oros D, et al. Study protocol for a randomised controlled trial: treatment of early intrauterine growth restriction with low molecular weight heparin (TRACIP). BMJ Open. (2018) 8(10):e020501.
12. Ngwenya S. Severe preeclampsia and eclampsia: incidence, complications, and perinatal outcomes at a low-resource setting, Mpilo Central Hospital, Bulawayo, Zimbabwe. Int J Women’s Health. (2017) 9:353–7.
13. Paauw ND, Luijken K, Franx A, Verhaar MC, Lely AT. Long-term renal and cardiovascular risk after preeclampsia: towards screening and prevention. Clin Sci. (2016) 130(4):239–46.
14. Iacobelli S, Bonsante F, Robillard P-Y. Pre-eclampsia and preterm birth in Reunion Island: a 13 years cohort-based study. Comparison with international data. J Matern Fetal Neonatal Med. (2016) 29(18):3035–40.
15. Ngwenya S, Jones B, Mwembe D, Nare H, Heazell AEP. Determinants of eclampsia in women with severe preeclampsia at Mpilo Central Hospital, Bulawayo, Zimbabwe. Pregnancy Hypertens. (2021) 25:235–9.
16. Fox R, Kitt J, Leeson P, Aye CYL, Lewandowski AJ. Preeclampsia: risk factors, diagnosis, management, and the cardiovascular impact on the offspring. J Clin Med. (2019) 8(10):1625.
17. Ananth CV, Lavery JA, Friedman AM, Wapner RJ, Wright JD. Serious maternal complications in relation to severe pre-eclampsia: a retrospective cohort study of the impact of hospital volume. BJOG. (2017) 124(8):1246–53.
18. Hidalgo-Lopezosa P, Cubero-Luna AM, García-Fernández R, Jiménez-Ruz A, Maestre-Luna MI, Liébana-Presa C, et al. Prevalence and mode of birth in late fetal mortality in Spain, 2016–2019. Int J Environ Res Pub Health. (2023) 20(3):1777.
19. Minhas AS, Rahman F, Gavin N, Cedars A, Vaught AJ, Zakaria S, et al. Cardiovascular and obstetric delivery complications in pregnant women with valvular heart disease. Am J Cardiol. (2021) 158:90–7.
20. Adeyinka DA. Geographical disparities in temporal trends of low birth weight in Saskatchewan from 2002/2003 to 2021/2022: insights from a joint point regression analysis. J Biosocial Science. (2024) 56(6):971–83.
© The Author(s). 2025 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.