Introduction
Ankyloblepharon filiforme adnatum may be secondarily presented with popliteal pterygium, which is a congenital defect that occurs rarely associated with cranio-facial, genitourinary, and extremity malformation. The clinical features vary with discrete combination of defect of palate, lip, pits in lower lip or sinuses, in which salivary ducts flow into, ankyloblepheron filiforme adnatum—partially or completely fusion of both eyelid margins with a thin band of tissues, and syngnathia—a congenital band of tissue between the maxilla and mandible (1–4). This syndrome is characterized by a band of connective tissue connecting ischial tuberosity and the calcaneus bone and also abnormal muscle insertion in lower extremity, which restricts the movement of leg in different directions (5). Moreover, digital deformities such as syndactyly, brachydactyly, and hypoplasia are also present. In one third of the cases, there is a triangular skin crease near the nail base of the hallux, which is considered almost a pathognomonic characteristic of this syndrome (6). In females, the majoral, the vaginal, and uterus hypoplasia but the clitoral hypertrophy are observed. In males, there may be cryptorchidism and absence of scrotum with the presence of normal penis. The intelligence of people with this syndrome is usually normal (6).
Research elaborations
A five-month-aged girl attended the pediatric outpatient clinic with the complaint of an inability to open both eyes and deformities in her face and legs since birth. Her prenatal, natal, and postnatal histories were unremarkable. She was the third baby of her parents and her milestone of development was normal according to age. On ocular examination, there was bilateral adhesion of both upper and lower lids with a thin band of tissue. The bands were at the middle and lateral third of the palpebral fissure and were outside of the lash line (Figure 1). Other ocular structures could not be seen due to the ankyloblepharon. Her weight was 6.7 kg. Her head circumference was 43 cm and the anterior fontanelle was 10 mm wide, which were normal for her age. There was a cleft defect of lip, palate, maxillomandibular fusion (syngnathia) on both side pterygium at popliteal fossa in both lower legs, with syndactyly in the right foot (Figures 1–3). There was hypoplasia of the labia majora and minora with normally developed clitoris. She was born to normal parents with no history of consanguineous marriage. Her siblings did not have any relevant ocular or systemic anomalies. She was diagnosed clinically as a patient with popliteal pterygium syndrome.

Figure 1. Ankyloblepheron filiforme adnatum, cleft Lip, and cleft palate.

Figure 2. Popliteal pterygium in both lower limbs.

Figure 3. Syndactyly in right foot.
Surgical technique
With all aseptic precautions and proper informed written consent from the legal guardian, the adhesive band was released with Westcott scissors under general anesthesia. Mild bleeding was managed by thermal cautery. Tobramycin 0.3% eye ointment was applied, and an eye patch was given for 3 h. The parents were advised to apply eye ointment twice daily for the next 7 days (Figures 4–6).

Figure 4. Ankyloblepheron filiforme adnatum just before surgery.

Figure 5. Just after surgery.
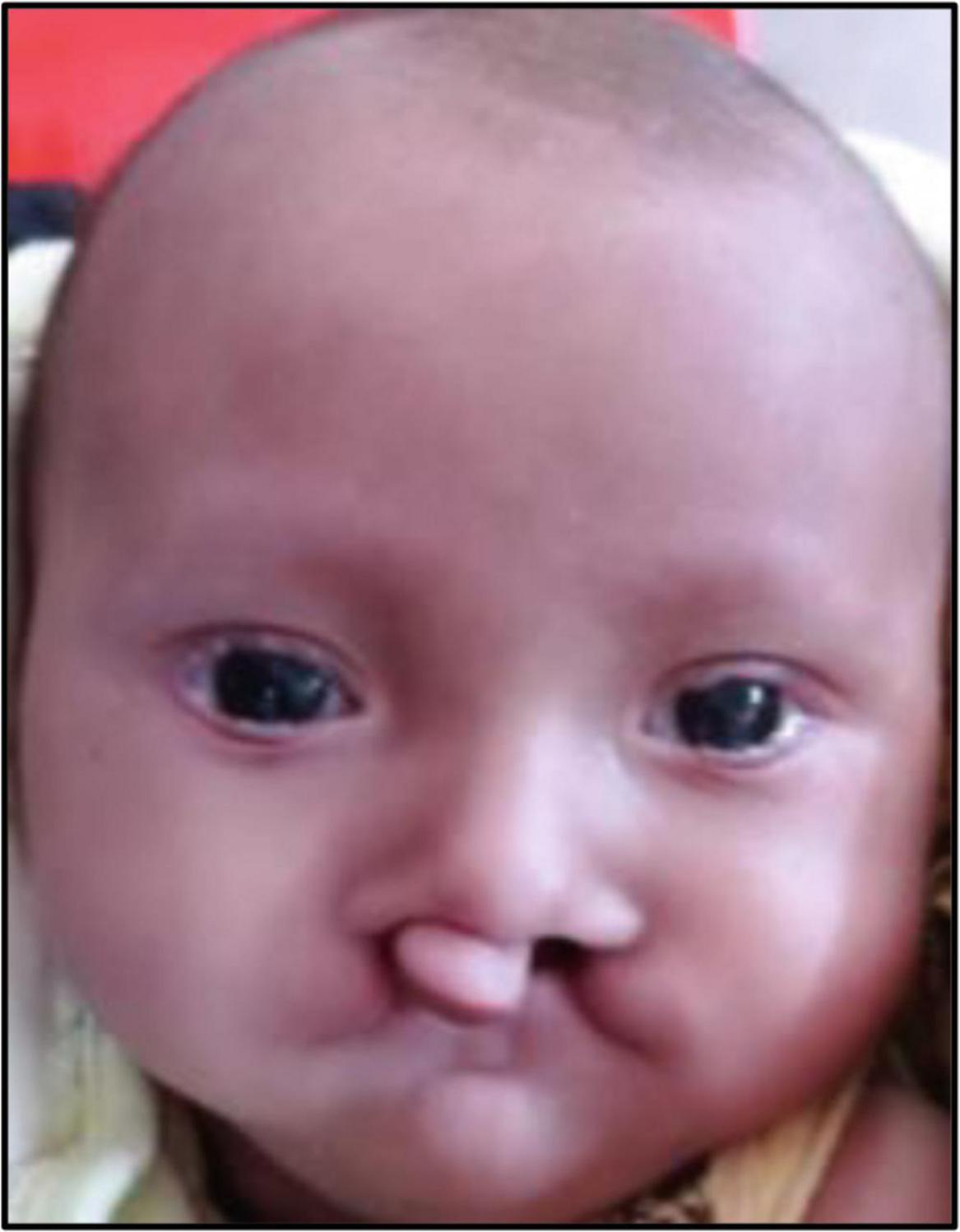
Figure 6. One day after surgery.
Discussion
Popliteal pterygium syndrome is a rare inborn disease with orofacial, cutaneous, musculoskeletal, and genital defects. It was first described by Trelat in 1869 and termed popliteal pterygium syndrome by Gorlin in 1969 (5). The frequency is one in 300,000 live births. It has no gender predisposition. Most of the reported cases are sporadic. Though rare, autosomal dominant transmission is also observed. In our case there was no positive family history, so it may be a sporadic case also. This anomaly is due to IRF6 gene mutation in the “q” arm of chromosome 1 (1q32.2). This gene encodes a transcriptional activator protein, called the interferon regulatory transcription factor (5). The pathophysiology of popliteal pterygium syndrome is still non-conclusive. Some researchers have suggested that disturbance of epithelial tissues, primarily due to microvascular abnormalities with edema, leads to the formation of secondary adhesion (6). People with this syndrome may have normal intelligence. There are some diagnostic criteria for popliteal pterygium syndrome like (1) cleft defect of lip and palate, (2) pterygium in the popliteal fossa, (3) lower lip sinuses, (4) abnormal genitalia, and (5) toe nail abnormalities. The presence of any three criteria is suggestive positive. Among these criteria cleft palate is the commonest, then cleft lip and popliteal webbing, lower lip sinuses, syndactyly, genitourinary abnormality, and nail abnormalities. (6) In the present case, she had cleft lip, cleft palate, and genitalia and toe abnormality with a normal milestone of development. The treatment for popliteal pterygium syndrome must be multidisciplinary, as it requires several surgeries. Surgeries for cleft lip and palate are started around 2 to 3 months of age and ocular surgery may start soon after birth to prevent amblyopia. In our case, the parent presented to the ophthalmologist at the age of 5 months and not yet started treatment for lip and palate abnormality. Ankyloblepheron filiforme adnatum can be managed by the simple excision of bands. In our case, lid adhesion was separated with Westcott scissors and mild bleeding was managed by thermal cauterization. Due to cleft lip and cleft palate, they have feeding difficulties; special measures may be needed to maintain nutritional support. Physical, occupational, and speech therapies are needed to improve the quality of life. Surgery can correct limb and facial abnormalities. Our patient was referred to a pediatric surgery specialist to take care of other anomalies and her parents were counseled on the importance of regular ocular follow-ups.
Conclusion
Ankyloblepheron filiforme adnatum presented with popliteal pterygium syndrome has multisystem deformities, which needed multidisciplinary approach to improve quality of life as well as for prevention of amblyopia.
Author contributions
MT: Literature review and manuscript writing. SR: Photography, manuscript review, and grammatical correction. S B: Concept, design, and manuscript preparation. NC: Manuscript review and grammatical correction. All authors contributed to the article and approved the submitted version.
Acknowledgments
We would like to thank Dr. Ahmadur Rahman Research Center.
References
1. Melnick M, Bixler D, Fogh-Anderson P, Conneally P. Cleft lip ± palate: an overview of the literature and an analysis of Danish cases born between 1941 and 1968. Am J Med Genet. (1980) 6:83–97.
2. Trelat U. Surune vice conformation tres rare de la levre inferieure. J Med Chir Prat. (1869) 40:442–5.
3. Gorlin RJ, Pindborg JJ, Cohen M. Syndromes of the head and neck. 2nd Edn. New York, NY: McGraw-Hill (1976).