Introduction
Type 2 diabetes mellitus (T2DM) is a major public health challenge globally, with older adults disproportionately affected due to age-related physiological changes, comorbidities, and long-term disease progression (1, 2). In Nigeria, the prevalence of diabetes among older adults is high, with recent estimates indicating that over 70% of this population is affected (3). Effective management of T2DM relies heavily on patients’ adherence to self-management practices, including medication adherence, blood glucose monitoring, physical activity, and dietary regulation (4, 5). Despite the critical role of self-management in glycemic control, older adults often face unique barriers, such as limited health literacy, economic constraints, and cognitive or physical impairments, which may compromise optimal disease management (6, 7).
Previous studies in Nigeria and other low-resource settings have reported suboptimal glycemic control among older adults with T2DM, yet the specific associations between glycemic outcomes and self-management behaviors remain underexplored (8, 9). Most available evidence is either hospital-based without national representation or focused on younger populations, leaving a critical gap regarding older adults, who are at increased risk of diabetes-related complications and mortality. Understanding these associations in the Nigerian context is particularly important given the country’s rising geriatric population and the unique socioeconomic and cultural factors influencing disease management.
This study, therefore, aimed to examine the association between glycemic control and diabetes self-management practices among older adults with T2DM across Nigeria’s six geopolitical zones. By employing a cross-sectional, nationally representative hospital-based design, the study sought to identify specific self-care behaviors that are most strongly associated with optimal glycemic outcomes in this high-risk population. The findings are expected to inform clinical practice, guide culturally tailored diabetes education programs, and support policy interventions aimed at improving glycemic control and reducing diabetes-related complications among older Nigerian adults. This study contributes to the field by providing evidence on (1) the prevalence of normal versus abnormal glycemic control among older adults with T2DM in Nigeria, (2) the self-management behaviors most strongly associated with glycemic outcomes, and (3) sociodemographic determinants influencing disease management, thereby addressing a critical knowledge gap in geriatric diabetes care in low-resource settings.
Methodology
Study design and setting
This study employed a hospital-based, cross-sectional design, justified by its feasibility in obtaining data from a geographically and demographically diverse sample within limited time and resource constraints. While this design allows the identification of associations, it does not establish causality; therefore, findings are interpreted as associative rather than causal. Data collection was conducted between August 2024 and September 2025 across 12 tertiary hospitals in Nigeria, carefully selected from the six geopolitical zones to ensure national representation. Each zone contributed two hospitals (one federal and one state-owned), recognized for their advanced diabetes care and specialized geriatric services.
Ethical approval
Ethical approval for the study was granted by the Federal Research Ethics Committee, and administrative authorization was obtained from the Chief Medical Directors of all participating facilities. The study adhered strictly to the ethical principles outlined in the Declaration of Helsinki and the American Psychological Association’s Ethical Principles for Research Involving Human Participants (10, 11). All participants provided informed consent, either in written form, orally, or via thumbprint, confirming voluntary participation without coercion or financial inducement. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (12).
Study participants
Eligible participants were older adults aged 60 years and above (mean age = 70.75 years) with a confirmed diagnosis of T2DM who attended outpatient diabetes clinics at the selected hospitals. Diagnosis was confirmed through medical records or physician verification. No new cases of diabetes were identified as part of the research process. Inclusion criteria comprised (1) age ≥ 60 years, (2) ability to provide informed consent, (3) cognitive and psychological soundness, (4) awareness of the hospital setting, (5) confirmed diagnosis of T2DM, and (6) being alive at the time of data collection. Individuals who did not meet these criteria were excluded.
Sampling procedure
A two-stage sampling technique was employed. In the first stage, Nigeria’s six geopolitical zones were defined as clusters, from which two tertiary hospitals (one federal and one state-owned) were purposely selected per zone, based on their specialization in diabetes management and patient volume. In the second stage, convenience sampling was used to recruit approximately 65 eligible older adults per hospital, targeting a total of 780 participants (13).
Sample size determination
The sample size was calculated using a 71.3% national prevalence of diabetes among older adults (3), applying the formula n = 40 DP/F2, where D = 71.3%, P = 28.7%, and F = 15% of D (10.7). Substituting these values yielded n = 40 × 71.3 × 28.7/114.5 = 700. To accommodate potential non-response (10%), an additional 70 participants were added, resulting in a final target sample of 780 participants. This sample size provided 80% statistical power to detect moderate associations at a 5% significance level (α = 0.05). Of the 780 eligible participants approached, 762 (97.7%) completed the survey, while 18 (2.3%) were excluded due to incomplete data. The low rate of missing data did not warrant imputation, and thus, listwise deletion was employed. Although the use of convenience sampling within hospital settings improved feasibility, it may limit the external validity and generalizability of the findings; this limitation is acknowledged in the Discussion section.
Data collection instrument
Data were obtained using the Glycemic Control and Diabetes Self-Management Questionnaire (GCDSMQ), a validated and reliable tool designed to assess sociodemographic characteristics, clinical variables, and diabetes self-management behaviors among older adults with T2DM. The instrument demonstrated strong internal consistency (Cronbach’s α = 0.88) (14). The GCDSMQ was developed and adapted from prior validated tools and empirical literature (4, 8, 15–17) and refined through expert consultation with nine doctoral-level public health professionals to ensure contextual and linguistic suitability for older Nigerian adults. The questionnaire was originally designed in simple English and translated into Yoruba, Hausa, and Igbo to accommodate participants’ language preferences. For respondents with limited literacy, trained interpreters provided real-time translation and assistance. A pilot test was conducted with 20 older adults who shared similar demographic and clinical characteristics to the target population, confirming the tool’s clarity, reliability, and cultural appropriateness. The questionnaire consisted of four major sections: Section A: Sociodemographic characteristics (age, gender, marital status, educational attainment, employment status, and living arrangement); Section B: Clinical characteristics (duration of diabetes and glycemic control); Section C: Diabetes self-management practices (including medication adherence, physical activity, glucose monitoring, and dietary behaviors); and Section D: Consent and participant acknowledgment.
Data collection procedure
Data collection was performed by 24 trained research assistants (two per hospital), all of whom were registered nurses employed at the respective sites. The principal investigator conducted a 35-minute structured training session to standardize the administration and interpretation of the questionnaire. The training covered ethical conduct, communication with older adults, and the management of participants with limited literacy. To maintain data quality and ensure consistency, several quality assurance strategies were implemented: (1) Structured role-playing exercises; (2) Supervised mock interviews; (3) Use of a standardized field operations manual; and (4) Continuous on-site supervision and spot-checks to monitor fidelity and inter-rater reliability. All questionnaires were administered during participants’ routine outpatient clinic visits to minimize inconvenience and avoid interference with clinical care schedules.
Data analysis
Data were analyzed using IBM SPSS Statistics for Windows, Version 22.0 (18). Descriptive statistics (frequencies and percentages) were used to summarize participants’ sociodemographic and clinical characteristics. Bivariate analyses were conducted using the chi-square (χ2) test to determine associations between glycemic control status (normal vs. abnormal) and categorical variables, including self-management practices and participant characteristics. For transparency, all χ2 values, degrees of freedom (df), and exact p-values were reported. To identify independent predictors of normal glycemic control, binary logistic regression analysis was performed. Predictor variables entered into the model included age, gender, marital status, educational qualification, employment status, living arrangement, and diabetes duration. Model diagnostics were conducted to ensure the reliability of the regression model. The Hosmer–Lemeshow goodness-of-fit test assessed overall model fit, while Variance Inflation Factor (VIF) values (<2.0) confirmed the absence of multicollinearity among predictors. A link test verified the correctness of the model specification. Adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were reported for each independent variable. Statistical significance was established at p ≤ 0.05.
Data quality and power considerations
Of the 780 distributed questionnaires, 762 were complete and suitable for analysis, reflecting a 97.7% response rate. Missing data accounted for less than 3% and were managed using listwise deletion, as the rate and pattern of missingness did not bias the analysis. The final analytic sample retained the 80% statistical power initially targeted, ensuring adequate sensitivity to detect moderate associations between glycemic control and self-management behaviors among older adults.
Results
Sociodemographic and clinical characteristics
A total of 762 participants were included in the study. The majority were aged above 70 years (57.9%), female (54.3%), and not currently married (60.9%). Most respondents held a university degree (71.4%), were retired or self-employed (69.9%), and lived with others (78.9%). More than two-thirds (67.7%) had lived with diabetes for five years or longer. Based on the most recent glycemic measurement, 62.9% had abnormal glycemic control, while 37.1% demonstrated normal control (Table 1).

Table 1. Sociodemographic and clinical characteristics of participants (N = 762).
Associations between glycemic control and diabetes self-management practices
Table 2 shows the associations between glycemic control status and diabetes self-management behaviors. Participants who reported regular blood sugar monitoring were significantly more likely to achieve normal glycemic control compared to those who did not (χ2 = 47.63, p < 0.001). Likewise, adherence to prescribed diabetes medication (χ2 = 55.67, p < 0.001) and engagement in physical activity for at least 30 minutes daily (χ2 = 33.79, p < 0.001) were significantly associated with normal glycemic control. Other self-management practices, including following a diabetes meal plan (p = 0.320), keeping regular medical appointments (p = 0.187), daily foot checks (p = 0.060), adjusting diet or activity based on glucose readings (p = 0.225), and correctly handling hypoglycemic or hyperglycemic episodes (p = 0.097), were not significantly associated with glycemic control.

Table 2. Associations between glycemic control status and diabetes self-management practices among participants (N = 762).
Bivariate associations between glycemic control and participant characteristics
As presented in Table 3, gender and employment status were significantly associated with glycemic control. A higher proportion of females achieved normal glycemic control compared to males (40.8% vs. 32.8%; χ2 = 4.54, p = 0.033). Similarly, glycemic control was better among those who were employed than among others (31.9% vs. 39.4%; χ2 = 4.07, p = 0.044). No statistically significant associations were found between glycemic control and age (p = 0.34), marital status (p = 0.33), educational qualification (p = 0.38), living arrangement (p = 0.86), or diabetes duration (p = 0.27).

Table 3. Bivariate associations between glycemic control status and participant characteristics (N = 762).
Multivariable logistic regression analysis
Results of the multivariable logistic regression are shown in Table 4. After adjusting for potential confounders, female gender remained significantly associated with higher odds of achieving normal glycemic control compared to males (OR = 1.41, 95% CI: 1.05–1.90, p = 0.033). Employment status was also significantly associated, as employed participants had lower odds of abnormal glycemic control compared to others (OR = 0.72, 95% CI: 0.52–0.99, p = 0.044). No statistically significant associations were observed for age (OR = 0.86, 95% CI: 0.63–1.17, p = 0.34), marital status (OR = 0.87, 95% CI: 0.64–1.18, p = 0.33), educational qualification (OR = 0.84, 95% CI: 0.61–1.15, p = 0.38), living arrangement (OR = 0.97, 95% CI: 0.68–1.39, p = 0.86), or diabetes duration (OR = 0.82, 95% CI: 0.60–1.12, p = 0.27).
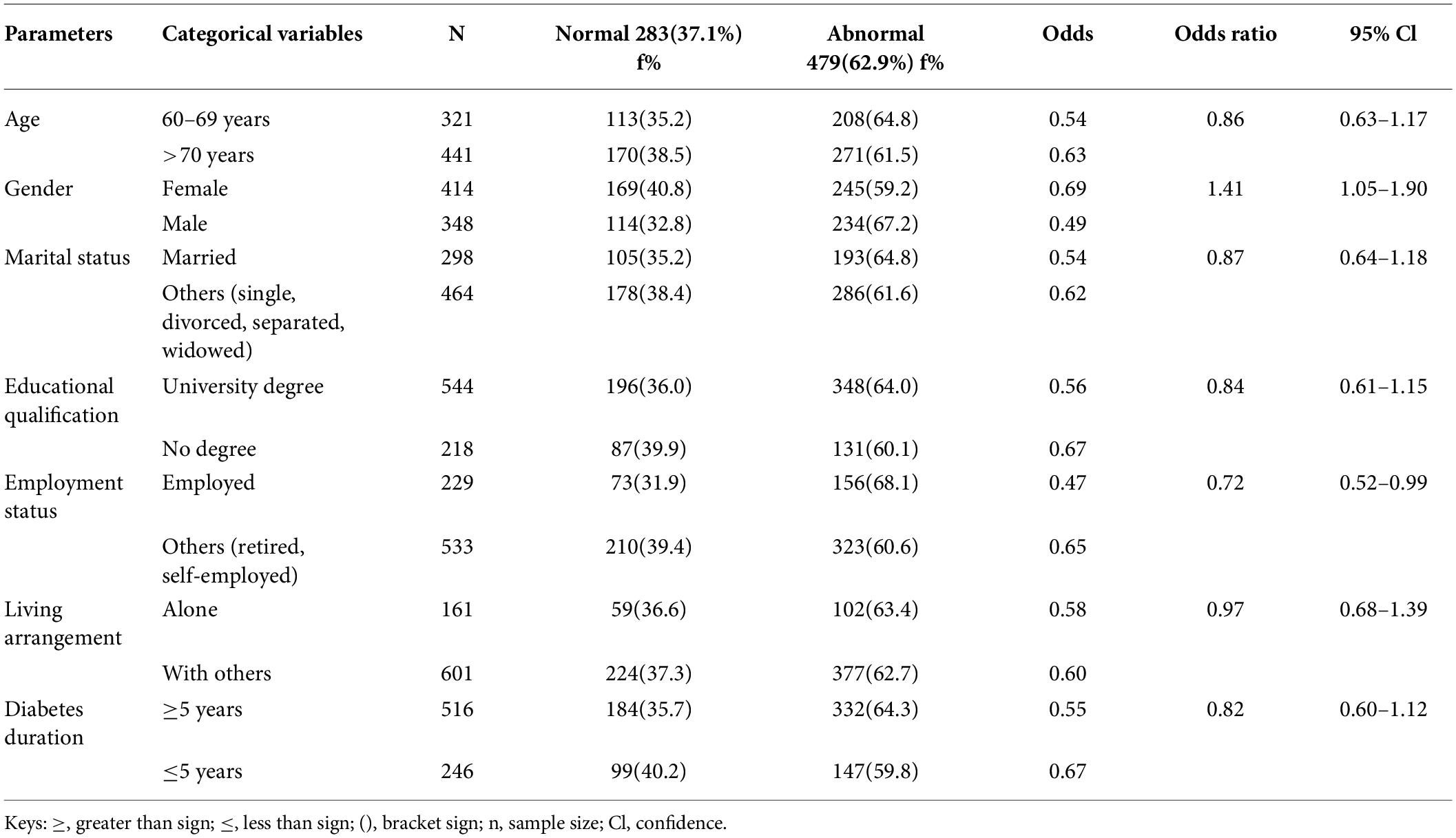
Table 4. Multivariable logistic regression analysis of factors associated with glycemic control status among participants (N = 762).
Discussions
This study explored the association between glycemic control and diabetes self-management practices among older adults with T2DM in Nigeria, offering insights into geriatric diabetes care in a low-resource, high-burden context. The findings revealed that, despite a high prevalence of abnormal glycemic control (62.9%), certain self-management behaviors, particularly medication adherence, regular blood glucose monitoring, and physical activity, were significantly associated with optimal glycemic outcomes. These findings have implications for clinical practice, public health policy, and stakeholder engagement in the management of T2DM among older adults in Nigeria and comparable low- and middle-income countries. The observed prevalence of abnormal glycemic control aligns with global trends, where older adults frequently exhibit suboptimal management due to multifactorial challenges, including physiological, cognitive, and socioeconomic factors (1, 2). The high proportion of participants with long-standing diabetes (≥5 years) underscores the chronic nature of the disease and its cumulative risk for complications, highlighting the urgent need for sustained self-management support and education (4, 5). Consistent with prior research, older adults with longer diabetes duration often struggle with maintaining glycemic control, partly due to progressive β-cell dysfunction, comorbidities, and polypharmacy (3, 19).
Medication adherence emerged as the most significant predictor of normal glycemic control, corroborating findings from multiple systematic reviews and cross-sectional studies in diverse settings (2, 9, 20, 21). Older adults face unique barriers to medication adherence, including complex regimens, cognitive decline, financial constraints, and limited health literacy (6, 7). The strong association observed in this study suggests that interventions targeting adherence, such as simplified dosing schedules, reminder systems, and caregiver involvement, could substantially improve glycemic outcomes in this population (5, 19). From a policy perspective, integrating structured adherence support into routine geriatric diabetes care could reduce hospitalizations and diabetes-related morbidity, aligning with global strategies for non-communicable disease management (1). Regular blood glucose monitoring was another self-management behavior significantly associated with optimal glycemic control. This finding is consistent with studies in both high- and low-resource settings, emphasizing the role of self-monitoring in enabling timely adjustments to lifestyle and medication (5, 15, 22, 23). Blood glucose monitoring provides immediate feedback on the physiological effects of dietary intake, physical activity, and medication adherence, thereby empowering older adults to engage in proactive self-management (2, 4, 24, 25). However, in low-resource settings like Nigeria, access to glucometers and test strips may be limited, necessitating targeted health policies that subsidize or improve the availability of monitoring tools (9, 19, 26).
Physical activity was also significantly associated with better glycemic outcomes. Engagement in at least 30 minutes of daily activity improves insulin sensitivity, reduces cardiovascular risk, and supports weight management in older adults (15, 20). Nevertheless, adherence to physical activity recommendations among older adults may be constrained by mobility limitations, fear of injury, comorbid conditions, and lack of safe environments for exercise (6, 7). These findings highlight the necessity for context-specific interventions, such as supervised group exercises, home-based activity programs, and community walking initiatives, which can enhance safety, motivation, and social support while promoting glycemic control (1, 5, 19). Contrary to expectations, other self-management behaviors, including dietary adherence, foot care, and adjusting lifestyle based on glucose readings, were not significantly associated with glycemic control in this study. Similar results have been reported in other African and low-resource contexts, suggesting that mere knowledge of self-care recommendations does not always translate into physiological outcomes (8, 21, 23). Dietary adherence, for instance, may be influenced by cultural dietary patterns, household food availability, and economic constraints, which can limit the effectiveness of recommended meal plans (9, 22, 27). These findings underscore the importance of culturally tailored diabetes education programs that consider economic realities, traditional diets, and caregiver involvement to improve adherence and subsequent glycemic outcomes (2, 5).
The significant association between female gender and glycemic control in this study aligns with some previous findings, which indicate that older women often exhibit better adherence to self-care behaviors, including medication use and clinic attendance, than men (8, 20). Sociocultural factors, such as gendered health-seeking behaviors, may contribute to these differences. Men, in contrast, may demonstrate lower engagement in preventive care and self-management, suggesting that gender-sensitive interventions, including male-targeted education and support programs, may be warranted to address disparities in diabetes outcomes (7, 9). Employment status also emerged as a significant determinant of glycemic control, with employed participants demonstrating lower odds of abnormal glycemia. Employment may confer multiple advantages, including financial security, routine structure, social engagement, and access to health benefits, all of which can facilitate adherence to self-management behaviors (6, 19, 28). Conversely, retired or unemployed older adults may face economic challenges that impede access to medications, glucose monitoring supplies, and healthy foods, highlighting the need for social protection policies and targeted subsidy programs for vulnerable populations (1, 9).
Interestingly, variables such as age, marital status, educational level, living arrangement, and diabetes duration were not significantly associated with glycemic control. While age is often considered a predictor of metabolic control due to physiological decline and comorbidity accumulation, our findings suggest that older adults in Nigeria may demonstrate heterogeneous self-management capacities, moderated by social support, health literacy, and access to healthcare services (3, 15). Similarly, educational attainment did not translate into improved glycemic outcomes, indicating that knowledge alone is insufficient without practical support, culturally adapted interventions, and healthcare accessibility (4, 5, 29–31). From a global public health perspective, these findings reinforce the need for integrative diabetes management approaches that combine pharmacological, behavioral, and social interventions. The observed high prevalence of suboptimal glycemic control further underscores this need.
This study’s strengths include its multisite, nationally representative design across Nigeria’s six geopolitical zones; a large sample size (n = 762) ensuring adequate statistical power; and the use of a validated, culturally adapted instrument with strong reliability (Cronbach’s α = 0.88). Rigorous training of research assistants, standardized data collection procedures, and high response rates (97.7%) enhanced data quality and internal validity. However, the hospital-based, cross-sectional design limits causal inference, and convenience sampling may reduce external generalizability to older adults not attending tertiary care facilities. Self-reported measures of diabetes self-management may also be subject to recall and social desirability biases.
Conclusion
This study examines diabetes self-management and glycemic control among older adults with type 2 diabetes in Nigeria, identifying key determinants of optimal outcomes. Medication adherence, regular glucose monitoring, and physical activity emerged as primary facilitators of normal glycemic control. Gender and employment status also influenced outcomes, emphasizing sociocultural and socioeconomic considerations in intervention design. The findings support structured, context-sensitive programs that enhance adherence, monitoring access, and safe physical activity. Targeted strategies addressing gender and socioeconomic disparities could further improve outcomes. Future longitudinal research should explore causal pathways and assess tailored interventions. Integrating culturally adapted education, digital support, and community resources may strengthen sustainable self-management and promote healthy aging in resource-limited settings.
Author contributions
All the authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Uchenna Cosmas Ugwu, Chuka Mackson Jones, Osmond Chukwuemeka Ene, Cordelia Chinonyerem Ugwu, Agatha Nneka Obayi, Christian Chukwuka Eze, and Blessing Amuchechi Omeh. The first draft of the manuscript was written by Uchenna Cosmas Ugwu and all the authors commented on previous versions of the manuscript. All the authors have read and approved the final manuscript.
Funding
No funding was received for conducting this study.
Acknowledgments
The authors sincerely acknowledge the Federal Research Ethics Committee and the Chief Medical Directors of all participating tertiary hospitals for granting ethical and administrative approvals. We are deeply grateful to the older adults who voluntarily participated in this study and generously shared their time and experiences. Special appreciation is extended to the 24 registered nurse research assistants across the 12 hospitals for their dedication, professionalism, and adherence to ethical and quality standards during data collection. We also thank the public health experts who provided valuable input during the development and validation of the questionnaire, as well as the hospital staff who facilitated smooth coordination of the study activities.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. World Health Organization. Diabetes. World Health Organization (2022). Available from: https://www.who.int/news-room/fact-sheets/detail/diabetes
2. Ahmad F, Joshi SH. Self-care practices and their role in the control of diabetes: a narrative review. Cureus. (2023) 15:e41409. doi: 10.7759/cureus.41409
3. Ugwu UC, Obayi AN, Ilo OO, Ene OC. Association between type 2 diabetes mellitus and bone mineral density in postmenopausal Nigerian women: a multicenter cross-sectional study. Disc Med. (2025) 2:253.
4. Bekele BB, Negash S, Bogale B, Tesfaye M, Getachew D, Weldekidan F , et al. Effect of diabetes self-management education on glycated hemoglobin (HbA1c) among patients with type 2 diabetes mellitus: a systematic review and meta-analysis of randomized controlled trials. Diabetes Metab Syndr Clin Res Rev. (2021) 15:177–85.
5. Powers MA, Bardsley JK, Cypress M, Funnell MM, Harms D, Hess-Fischl A , et al. Diabetes self-management education and support in adults with type 2 diabetes: a consensus report. Diabetes Educ. (2020) 46:350–69.
6. Adhikari M, Devkota HR, Cesuroglu T. Barriers to and facilitators of diabetes self-management practices in Rupandehi, Nepal: multiple stakeholders’ perspectives. BMC Public Health. (2021) 21:1269.
7. Awang Ahmad NA, Sallehuddin MAA, Teo YC, Abdul Rahman H. Self-care management of patients with diabetes: nurses’ perspectives. J Diabetes Metab Disord. (2020) 19:1537–42.
8. Ugwu UC, Ene OC. Knowledge, attitude, and practice towards diabetes mellitus among outpatient diabetic elderly persons: a descriptive study. Int J Diabetes Dev Ctries. (2021) 42(3). doi: 10.1007/s13410-021-00948-2
9. Opoku R, Ackon SK, Kumah E, Botchwey CO, Appiah NE, Korsah S , et al. Self-care behaviors and associated factors among individuals with type 2 diabetes in Ghana: a systematic review. BMC Endocr Disord. (2023) 23:256.
10. World Medical Association. Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. (2013) 310:2191–4.
11. American Psychological Association. Ethical Principles of Psychologists and Code of Conduct. American Psychological Association (2017).
12. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. (2007) 335:806–8.
15. Garedow AW, Jemaneh TM, Hailemariam AG, Tesfaye GT. Lifestyle modification and medication use among diabetes mellitus patients attending Jimma University Medical Center, southwest Ethiopia. Sci Rep. (2023) 13:4956. doi: 10.1038/s41598-023-31990-1
16. National Population Commission (Npc) [Nigeria], Icf. Nigeria Demographic and Health Survey 2018. NPC & ICF (2019). Available online at: https://dhsprogram.com/pubs/pdf/FR359/FR359.pdf
17. American Diabetes Association. Standards of care in diabetes—2023. Diabetes Care. (2023) 46(Suppl 1):S1–291.
18. IBM Corporation. IBM SPSS Statistics for Windows (Version 28.0) [Computer Software]. IBM Corp. (2021).
19. Lamptey R, Amoakoh-Coleman M, Djobalar B, Grobbee DE, Adjei GO, Klipstein-Grobusch K. Diabetes self-management education interventions and self-management in low-resource settings: a mixed-methods study. PLoS One. (2023) 18(6):e0286974. doi: 10.1371/journal.pone.0286974
20. Chenchu Karthik R, Radhakrishnan A, Vikram A, Arumugam B, Jagadeesh S. Self-care practices among type II diabetics in a rural area of Kancheepuram District, Tamil Nadu. J Family Med Prim Care. (2020) 9:2912–8.
21. Chinnappan J, Athira KP, Iqbal F, Jasna V, Ashok P, Varghese RS. Assessment of self-care practices among type 2 diabetic patients in a secondary care teaching hospital. J Drug Deliv Ther. (2020) 10:119–24.
22. Mohammed AS, Adem F, Tadiwos Y, Woldekidan NA, Degu A. Level of adherence to dietary recommendations and glycemic control among patients with type 2 diabetes mellitus in Eastern Ethiopia: a cross-sectional study. Diabetes Metab Syndr Obes. (2020) 13:2605–12.
23. Uloko AE, Musa BM, Ramalan MA, Gezawa ID, Puepet FH, Uloko AT , et al. Prevalence and risk factors for diabetes mellitus in Nigeria: a systematic review and meta-analysis. Diabetes Ther. (2018) 9:1307–16.
24. Loerbroks A, Nguyen XQ, Vu-Eickmann P, Krichbaum M, Kulzer B, Icks A , et al. Psychosocial working conditions and diabetes self-management at work: a qualitative study. Diabetes Res Clin Pract. (2018) 140:129–38.
25. Stephani V, Opoku D, Beran D. Self-management of diabetes in Sub-Saharan Africa: a systematic review. BMC Public Health. (2018) 18:1148. doi: 10.1186/s12889-018-6050-0
26. Lambrinou E, Hansen TB, Beulens JWJ. Lifestyle factors, self-management and patient empowerment in diabetes care. Eur J Prev Cardiol. (2019) 26:55–63.
27. Briggs Early K, Stanley K. Position of the Academy of Nutrition and Dietetics: the role of medical nutrition therapy and registered dietitian nutritionists in the prevention and treatment of prediabetes and type 2 diabetes. J Acad Nutr Diet. (2018) 118:343–53.
28. Bonger Z, Shiferaw S, Tariku EZ. Adherence to diabetic self-care practices and its associated factors among patients with type 2 diabetes in Addis Ababa, Ethiopia. Patient Prefer Adherence. (2018) 12:963–70.
29. Zhao F, Suhonen R, Katajisto J, Leino-Kilpi H. The association of diabetes-related self-care activities with perceived stress, anxiety, and fatigue: a cross-sectional study. Patient Prefer Adherence. (2018) 12:1677–86.
30. Mogre V, Abanga ZO, Tzelepis F, Johnson NA, Paul C. Adherence to and factors associated with self-care behaviours in type 2 diabetes patients in Ghana. BMC Endocr Disord. (2017) 17:20.
31. Ugwu UC. Digital health technology adoption among older Nigerian adults with type 2 diabetes mellitus: a hospital-based cross-sectional study. J Diabetol. (2026). doi: 10.4103/jod.jod_127_25
© The Author(s). 2025 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.