Introduction
There is no argument that diarrhea, as one of the leading causes of death, especially under-five age children mortality globally, has persisted over the years despite efforts to eradicate it. It is on record that diarrhea is one of the leading causes of death of children under age five that is responsible for killing around 443,832 under-five children and an additional 50,851 children within the age bracket of 5–9 years annually (1, 2). Record also has it that in the year 2016 alone, there were an estimated 4.5 billion episodes of diarrhea globally, with diarrhea ranking eighth among the leading causes of death worldwide, accounting for more than 1.6 million deaths among all ages and being the fifth leading cause of death among under-five children (3). It is obvious that it is not only children under five years of age that die through diarrhea, even though they are more at risk of dying by diarrhea than any other age group; individuals from other age categories also do die through diarrhea.
It is not as if there have not been improvements over the past two decades, but the challenge is that progress has remained slow (2). In fact, in spite of the advancements in Africa, diarrheal diseases keep posing a significant public health challenge that continues to affect vulnerable populations like children under age five disproportionately due to limited access to clean water, sanitation, and adequate healthcare resources, causing high rates of morbidity and mortality (4–6). In sub-Saharan Africa, record have it that there are more than one billion diarrheal episodes and an estimated 606,024 diarrheal deaths annually, with almost half of the deaths occurring in children under age five (3). The authors also reveal that approximately 90% of all diarrheal deaths occur in South Asia and sub-Saharan Africa.
From WHO’s (2) perspective, diarrhea denotes the passage of three or more loose or liquid stools per day (or more frequent passage than is normal for the individual). This excludes frequent passing of formed stools and the passing of loose, pasty stools by breastfed babies (2). In a Nigerian parlance, someone experiencing a loose stool is said to be having a running stomach; it is common to people of all ages and normally stops after a few days, but if it persists for more than three days or the person experiences other symptoms like fever, serious headache, or bloody stool, it becomes advisable for such a person to visit a health practitioner, especially a medical doctor. To Nemeth and Pfieghaar (7), diarrhea is a common condition that varies in severity and etiology. The authors aver that its evaluation varies depending on the duration, severity, and presence of certain concurrent symptoms.
The causes of diarrhea are varied, and it ranges from infections, food poisoning, food intolerance, and/or medications. In a more specific note, diarrhea is usually a symptom of an infection in the intestinal tract that can be caused by a variety of bacterial, viral, and parasitic organisms, and the infection is spread through contaminated food or drinking water or from person to person as a result of poor hygiene (2). More so, diarrheal disease can spread from person to person, aggravated by poor personal hygiene; food prepared or stored in unhygienic conditions; unsafe domestic water storage and handling; and fish and seafood from polluted water (2). In fact, such factors as age-related vulnerabilities, gender disparities, maternal education, maternal occupation, the method of stool disposal by young children, water availability and quality, economic influences, and environmental factors collectively play a role in the prevalence of diarrheal diseases (4–6). Besides, poverty, characterized by limited access to vital resources such as clean water, sanitation, and healthcare, tends to be a serious issue in diarrheal diseases (4, 6).
The good thing, though, is that a significant proportion of diarrheal diseases can be prevented through improvement in drinking water and adequate sanitation and hygiene (2, 8). This underscores the importance of the provision of basic social amenities and its contributions in reducing death by diarrhea. Merid et al. (9) opine that improved water and sanitation had a larger impact on the reduction of diarrheal disease than improvement in water or sanitation alone and emphasized that achieving Sustainable Development Goal 6 (SDG 6) is germane to the reduction of diarrhea among rural children below the age of five. Similarly, Mohamed (10) asserts that the primary factors in the reduction of under-five mortality rate in Sudan were improvements in access to safe water, sanitation, and hygiene (WASH) and basic education and emphasized that failures in the provision of WASH services and inclusive basic education could have a negative effect on achieving the improvement in child health as contained in SDG 3.2. Similarly, Nwokoro et al. (3) argue that increasing access to improved sanitary sewage disposal methods and promoting hand-washing with soap and water at critical moments are capable of improving diarrheal disease control in Enugu, South-East Nigeria.
It is, therefore, upon these premises that this study focused on the views of people regarding the effect of the provision of basic social amenities and deaths by diarrhea in South-East Nigeria. This is capable of pushing the governments towards living up to their responsibilities and working hard to achieve the Sustainable Development Goals (SDGs)—one (no poverty), two (zero hunger), three (good health and well-being), four (quality education), and six (clean water and sanitation)—in the area of study.
Objective
This study has just one specific objective, which is to:
1. Examine the relationship between the provision of basic social amenities and deaths by diarrhea in South-East Nigeria.
Research questions
1. What is the relationship between the provision of basic amenities and deaths by diarrhea in South-East Nigeria?
Research hypothesis
1. There is no significant relationship between the provision of basic social amenities and deaths by diarrhea in South-East Nigeria.
Conceptual clarifications/literature review
Basic social amenities
Basic social amenities are things considered to be essential to make life easier and more pleasant or enhance quality of life, such as clean water, sanitation, healthcare, electricity, education, recreational facilities, drainage, pipe-borne water, toilets, personal washing facilities, or cooking facilities (11). In fact, Rebecca (11) views the provision of these amenities as the responsibility of the government and a fundamental human right. It is also not wrong to talk about the link between basic social amenities and death by diseases. For example, poor medical attention and hygienic conditions during delivery (12) and hunger or lack of good food (13) all affect people’s quality of life, thereby increasing rates of death by communicable diseases, diarrhea inclusive.
World Health Organization (WHO) (14) noted that the poor are more susceptible to ill health than the well-off because they lack safe water supplies and safe methods of disposing of their waste. This observation further shows that where a community improves its water supply, hygiene, and sanitation, then health improves. For example, diarrhea can be reduced by 26% when basic water, hygiene, and sanitation are supplied. Besides, poor medical attention and hygienic conditions during delivery (15–17).
Death
Death is inevitable to all living things; in human society everyone dies. The only difference is the circumstances of the death, as it could come through accident, suicide, the aging process, or diseases and infections. Haralambos and Holborn (18) argue that sociology’s original and most famous study of death is Durkheim’s Suicide, in which Durkheim maintained that death is best understood in a context. It has different meanings to different people.
Tomasini (19), for example, sees death (biological death) as a total event, an absolute state, and a part of the dying process; and this differs from the ideas of Leming and Dickinson (20) and Scarre (21) that death occurs when an individual has sustained either irreversible cessation of circulatory and respiratory functions or irreversible cessation of all functions of the entire brain, including the brain stem. In fact, Tomasini (19) argues that the definition did not capture the irreversible final moment of death. Moreover, Fabis and Kilimczuk (22) see death as a state of the total disappearance of life and dying as a process of decay of the vital system, which ends in clinical death, but acknowledge that there are current approaches to the definition of death. Walter (23), in his work, “The Sociology of Death, Dying, and Bereavement,” explores and interrogates the relationship between society and death. Baloyi (24) states that in African perceptions and cultural inclinations, death is but a transition from the visible to the invisible spiritual ontology. To Nnoruga (25), death is considered a scary phenomenon among many people of different cultures of Africa, and many things are done to prevent it. In all, death is a phenomenon that brings a lot of grief to humanity, and humans are involved in one way or another.
Diarrhea
Diarrhea, from the perspective of Cleveland Clinic (26), is having a loose stool during a bowel movement of defecation, as some would term it. It can also be defined as a passage of three or more loose or liquid stools in less than 24 hours, or more frequent passage than the individual is used to (9, 27). As already captured in this study, Nemeth and Pfieghaar (7) view diarrhea as a common condition that varies in severity and etiology, and its evaluation varies based on the duration, severity, and presence of certain concurrent symptoms. WHO (2) states that diarheal disease is the third leading cause of death in children 1–59 months of age; it kills about 450,000 children under the age of five every year.
Diarrhea is a leading cause of malnutrition in children under five years old through a variety of mechanisms involving loss of nutrients in stools and vomitus, increased metabolic demand, and poor appetite, and malnutrition contributes to about half of the deaths in children under age five (2, 27). Atimati and Eki-Udoko (27) argue that diarrhea-related death can be associated with severe dehydration and electrolyte derangement, but bacterial sepsis seems to contribute to death with rising frequency. The authors further argue that diarrhea is caused by gastrointestinal tract infection caused by microorganisms (viruses, bacteria, and parasites) from contaminated food and water (27). In all, it is obvious that one can be infected with diarrhea when one drinks unsafe water, lives in a dirty environment, and does not practice personal hygiene, as these could be avenues of transmitting the causative organism of diarrhea to the gastrointestinal tract.
Theoretical framework
Demographic transition theory, especially the first and second stages, was appropriate in the explanation of socio-economic aspects of deaths by diseases in the area of study. The first stage of the transition involves high birth rates, and death rates and the countries that fall into this category are found mainly in Africa, Asia, and South America; and the high death rates are caused by diseases and undernourishment, famine, wars, epidemics, etcetera (28).
Applying this to the study of mortality in Nigeria, it is common knowledge that Nigeria, as the giant of Africa, is characterized by high birth and death rates. The high mortality rates in Nigeria, just like in other developing countries, are likely caused by diseases and chronic undernourishment, epidemics, famine, wars (i.e., crises, conflicts, military interventions, terrorists’ activities, etc.), etcetera. In agreement with this view with reference to Nigeria, Fasan (29) asks, “How can a civil servant who can’t pay his daughter’s medical bill for a disease caused by the very fact of their material poverty bear the ill-digested platitude of a state governor calling for cooperation between him and the mass of hungry people around?” This shows that hunger, famine, and material poverty occasioned by low-level education, unemployment, underemployment, and inadequate basic social amenities are still common in Nigeria to the extent that many families are unable to pay hospital bills for their infected children, and the outcome of this will definitely be high disease and death rates.
Stage two is associated with high birth rates and low death rates. The causes of the rapid drop in death rates are improvement in food supply and sanitation, access to technology, improvement in healthcare and education, feminine techniques, crop rotation, and selective breeding (28, 30). In Nigeria, there is evidence of improvement in sensitization and disease awareness, sanitation, etcetera. For example, the introduction of sex education and other disease awareness programs into the school curriculum will definitely lead to a drop in death rates in Nigeria, as reported by NPC & ICF Macro (31). But death rates are still high despite its downward trend, showing that ignorance is not the major issue, but low quality of education is the issue.
Nigeria has not gotten to the third stage, just like their counterparts in sub-Saharan Africa, as its birth and death rates are still relatively high (32). This agrees with Adetunji and Bos (33) that sub-Saharan Africa is the region of the world with the highest level of mortality (death), with the overall life expectancy at birth of 46 years.
Methodology
Design
This study adopted a cross-sectional survey design. This design is cost-effective in a study of this nature that involves large population, and it will enable the researcher to gather data at one point in time within a limited time frame.
Area of the study
This study was carried out in South-East Nigeria. This area is one of the six geopolitical zones in Nigeria. Others are North-East, North-West, North-Central, South-West and South-South. The South-East Nigeria is made up of five states namely Abia State, Anambra State, Ebonyi State, Enugu State, and Imo State. It is an Igbo speaking zone with 95 local government areas (LGA) that cut across its five states (Abia State 17 LGAs; Imo, 27; Ebonyi, 13; Anambra 21 and Enugu, 17), and the majority of its people are Christians.
The socio-cultural organization of the South-Eastern people of Nigeria is mainly based on membership in kinship groups and parallel but complementary dual-gender associations which are important to societal integration. The associations take several forms including age grades, men’s societies, women’s societies, and prestige-title societies such as “Nze” or “Ozo” for men and the “Omu”, “Ekwe”, or “Lolo” for women. The interaction among these groups prevents the concentration of authority in any one association (34).
Population of the study
The total population of South-East Nigeria based on 2006 National Population and Housing Census is 16,395,555 people (8,184,951 for male and 8,210,604 for female). The population is further projected to 28,007,927 people distributed by gender and states on Table 1.

Table 1. Projected population of South-East Nigeria by gender and states.
The target population for the study, however, was 10,408 persons, being the population of some six (6) relevant population categories for this study, which cut across the study area. The population categories were as follows: men, women, youths, teachers, health workers, and religious leaders. The target population is shown in Table 2.
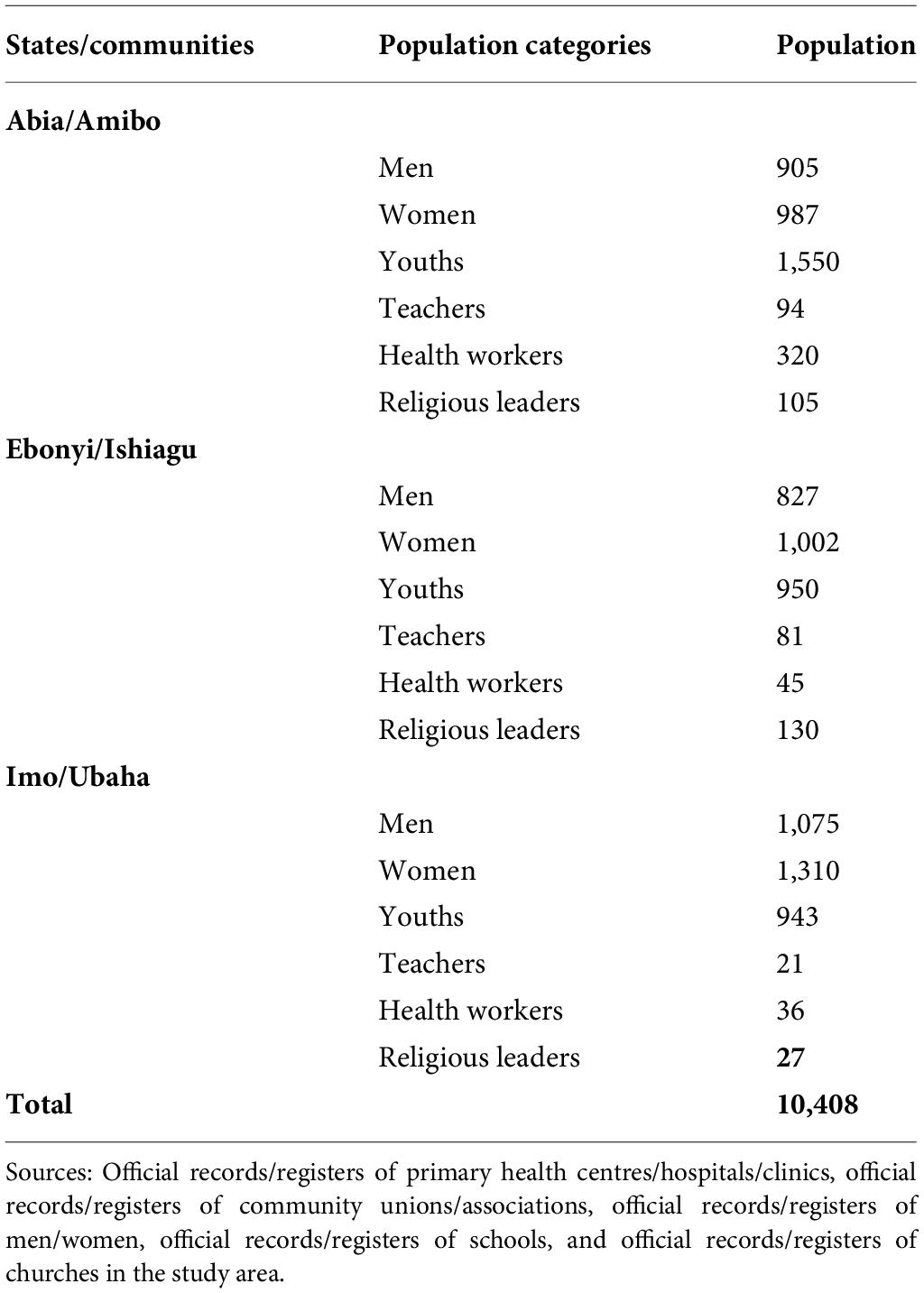
Table 2. Target population for the study.
Scope of the study
The study was limited to livelihood issues in deaths by diseases in South-East Nigeria focusing on Abia, Ebonyi, and Imo states. The states were selected by simple random sampling.
Sample size
The sample size for this study was 590 persons. This was statistically generated by using Taro Yamane’s statistical method of determining sample size as follows:
where: n = Sample size
N = Target Population
e = error of sample (it could be 0.10 down to 0.01, but in this work, 0.04 was used)
1 = unity or constant
Therefore
Sampling technique
Multi-stage stratified cluster sampling is adopted. First, three out of the five states were selected. The five states were numbered, and three out of the five were selected. The selected states are Abia, Ebonyi, and Imo states. Next, three LGA, one from each of the selected states, were selected. All the LGA in each of the selected states were numbered, and one was selected from each state, making it a total of three LGA. The selected LGA are Umuahia-South (Abia State), Ivo (Ebonyi State), and Okigwe (Imo State). Furthermore, all the communities in each of the selected local governments were numbered, and one was selected from each of the LGAs, making it a total of three communities. The selected communities are Amibo (Umuahia-South, Abia State), Ishiagu (Ivo, Ebonyi State), and Ubaha (Okigwe, Imo State). In order to collect appropriate data for the study, six relevant population categories were created in each community. The members of each population category formed the respondents for the study. The stratified proportionate sampling technique was used in selecting the respondents from each population category in view of the fact that the population categories did not have equal size. The availability sampling technique was used to select the actual respondents from each population category, as shown in Table 3.

Table 3. Proportionate stratified random sampling technique for the study.
For the qualitative data [in-depth interview (IDI) data], 15 people were purposively selected for interview, 5 from each of the 3 communities, based on their leadership positions in the relevant qualitative population categories as follows:
1. Three titled men (one from each of the communities)
2. Three women leaders (one from each of the communities)
3. Three youth leaders (one from each of the communities)
4. Three doctors/senior matrons (one from each of the communities)
5. Three head teachers/principals (one from each of the communities)
Instruments for data collection
The instruments for data collection of this study were a questionnaire and IDI because of the need for mixed-method research (in this case, 50% quantitative and 50% qualitative) for an investigation on livelihood issues in deaths by diseases in South-East Nigeria. The questionnaire, specifically, was used to collect quantitative data, and it was highly structured with only a few unstructured questions. It also had two different sections. The first section contained the socio-demographic characteristics of respondents, while the other sections addressed the substantive issues in livelihood factors and deaths by diseases in South-East Nigeria.
The IDIs, on the other hand, were employed to gather qualitative data to complement the quantitative data for deeper, understanding of the livelihood issues in deaths by diseases in the study area. The IDIs were anchored mainly on unstructured questions with necessary probes.
Administration of instrument
The questionnaire was administered by the principal researcher himself and his three research teammates with the help of four research assistants. The research assistants were recruited on the basis of their ability to read and write and speak and understand both English and the local dialects of the communities. They were people (males and females) that hail from either the communities or LGAs of the study. They were trained for 3 days on the objectives of the study, the relevance of the study, and the administration and retrieval of questionnaire. The IDIs were conducted by the researcher and three research teammates only.
Method of data analysis
The quantitative data collected through the questionnaire were processed with Statistical Package for Social Sciences (SPSS) Version 20.0. The socio-demographic characteristics of respondents and the substantive issues in all sections of the questionnaire were analyzed using descriptive statistics such as simple frequency distribution tables, percentages, graphs, and charts. Inferential statistics, particularly, logistic regression, pearson moment correlation coefficient, and multiple regression analysis, were used to test the stated hypotheses and predict the relationship between the independent and dependent variables.
Results
Out of 590 copies of the questionnaire distributed, only 555 (94.07%) copies were retrieved and valid, while 35 (5.93%) were either not retrieved or invalid.
Table 4 provides a descriptive summary and interpretation of the demographic data collected from the sample population of the study. The variables covered include age, gender, marital status, educational qualification, occupational status, and annual income.

Table 4. Socio-demographic characteristics of respondents (N = 555).
The age group most represented in the sample is 42–49 years, accounting for 42.9% of respondents. This is followed by the 34–41 years group (13.9%). The 18–25, 26–33, 50–57, and 58–65 age groups each constitute approximately 9%–10% of the population, while the 66 and above category is the least represented (5.8%). The data suggests that a majority of the respondents are middle-aged, indicating that this age group may be the most active or engaged within the context of the study.
The gender distribution is relatively balanced, with a slight male predominance. This suggests a near-equal representation of perspectives from both genders. A significant portion of the population, 297 (53.5%), is married, which may influence their economic responsibilities, purchasing behavior, or social outlook.
The highest proportion of respondents 143 (25.8%) possess a First School Leaving Certificate, followed by those with O’ level education 120 (21.6%) and First Degree holders 113 (20.4%). A notable 98 (17.7%) have no formal education, while only 29 (5.2%) possess postgraduate qualifications (MSc/PhD). The educational profile leans towards basic and secondary education, indicating a potential gap in higher-level skills and literacy that may affect employment opportunities or access to information.
The high representation of business people, 190 (34.2%), and public servants, 159 (28.6%), suggests a diversified workforce, with a strong presence in both formal and informal economic sectors. Income distribution indicates that most respondents are earning a moderate to high income (that is, between 50,000–74,999 and 100,000 and above), potentially reflecting economic stability among the surveyed population, especially among public servants and business owners.
This demographic data highlights a mature, moderately educated, and economically active population. With a majority engaged in business or public service and earning a relatively high income, the findings suggest a group with potential societal influence. However, the notable proportion with low or no formal education may suggest areas for targeted policy intervention in education and vocational training.
Analysis of substantive issues
Research questions 1
What is the relationship between the provision of basic amenities and deaths by diarrhea in South-East Nigeria? The responses to this question are presented in Tables 5–7.

Table 5. Bereavement experience and cause of death (N = 555).

Table 6. Living conditions of deceased from diarrhea (N = 52).

Table 7. Sanitary conditions of deceased residence.
Table 5 shows the bereavement experiences of the respondents and the causes of death in the area of study. The data show that 372 (67%) of the 555 respondents reported having experienced bereavement in the past year to the time of the fieldwork for this study in 2025 due to communicable diseases, while 183 (33.0%) have not experienced such bereavement in the recent time. This shows that more than two-thirds of the respondents had been bereaved recently. This corroborated the IDI data, as more of the IDI respondents admitted that they have experienced bereavement at present.
With regard to the specific causes of the deaths (i.e., the specific communicable diseases), the data in Table 5 also show that more deaths, 130 (34.9%), occur in South-East Nigeria from malaria followed by typhoid, 98 (26.3%), and other causes, 92 (24.7%), which most likely include kidnapping, banditry, road accidents, and heart attacks. This shows that malaria and typhoid are major contributors to the loss of loved ones in South-East Nigeria. This also corroborated the qualitative data.
This shows a majority of the respondents have lost someone to a communicable disease, suggesting a high burden of disease-related mortality within South-East Nigeria. In fact, these insights highlight the urgent need for public health interventions involving improved disease prevention, sanitation, access to healthcare, and education in South-East Nigeria.
Table 6 shows that a majority of the deceased, 230 (61.8%), lived in communal residences, suggesting a high prevalence of shared or multi-occupancy housing units; 102 (27.4%) resided in open streets, which may indicate informal or less structured living arrangements; 24 (6.5%) lived in quarters, while 16 (4.3%) lived in estates. The data indicates that a majority of the deceased resided in environments that are likely to be densely populated and may have limited access to private amenities. This corroborated the qualitative data, as more of the deceased were reported to have lived in communal residences before their deaths.
The data in Table 6 also show that the most common housing types among the deceased were bungalows (140 deceased, 37.6%) and two-room block houses (134 deceased, 36.0%). These figures suggest that a significant proportion, 274 (73.6%), of the deceased had access to more stable housing structures, while a combined total of 47 deceased (12.6%) lived in more basic housing units, which included mud houses (22 respondents, 5.9%) and one-room block houses (25 respondents, 6.7%), which may reflect lower-income households. Only a minority, 31 (8.3%) and 20 (5.4%), of the deceased lived in flats and duplexes, respectively, and this possibly indicates a better socioeconomic status among a small segment of the population. This corroborated the qualitative finding, as one of the IDI respondents rightly noted:
We have bungalows, we have skyscrapers here, I don’t know. It is rare to see mud houses here in this Ubahu. You can’t! People are just upgrading; you cannot see mud houses. The least you see here are bungalows, and that’s what a lot of people live in, even the person I lost (female, Nurse, 52 years old, Imo State).
No…People in the Isiagu community don’t actually have bad houses because their children have grown up to…I don’t think if there is a mud house, it should be at a low rate; people are now building houses where they put modern toilets and the rest (female, student, 21 years old, Ebonyi State).
Like, you can see my own, nah, you can snap it. If you go to the main road, you will see beautiful houses; we are civilized. You don’t talk of thatch houses in Ubahu here. There are only a few old family houses living in “face-me-I-slap you” but not mud houses. The houses here are mainly bungalows (female, civil servant/farmer, 47 years old, Imo State).
Well, you know that when it comes to housing, this community is somehow civilized; the majority are living in good houses, and only very few are living in bad houses because of poverty. Um…the majority live in, let me call it a bungalow not duplex. Yes, a bungalow (male, teacher, aged 50 years, Imo State).
The data also show that a majority of the bereaved 240 (65.6%), reported that the deceased had access to water system toilets, relatively reflecting their conversance with modern sanitation facilities, while a combined 128 (34.4%) practiced open defecation and used general/shared toilets, respectively, thereby highlighting critical gaps in sanitation infrastructure that need to be addressed to improve public health outcomes. This finding also corroborated the IDI data. One of the IDI respondents noted:
…even in this community, we don’t have latrines again; people now use the water system…Everybody now uses a water system, but the problem there is keeping it clean; washing it, when washed, prevents all these diseases and their resultant deaths. The only people that engage in open defecation are residents of commercial houses. They will leave their house, and they will go to the bush to defecate. I don’t know their reasons (female, nurse, 52 years old, Imo State).
Toilet facilities: most people use the modern system of toilet, that is, the Water Closet (WC). Like my grandma now, she doesn’t even go to the toilet; she goes to the bush and uses leaves to clean her anus. All these things, they are giving her bacteria, but when you tell her, she will not listen to you; she will say that the best place she wants to the going to toilet…From my assessment, however, people use more of WC (female, student, 21 years old, Ebonyi State).
Yes, like myself, I have a good toilet. Right now we are civilized; everybody has a water system. We are village township people. Just like me now, I have a water system; I don’t have a pit toilet. I doubt it could be few out of that, that’s one out of a hundred. We are civilized, ooo! If there were no good toilets and other basic facilities here, maybe I could have been telling you now that more people are dying of diarrhea in this community. It was when I was not married that we were using those old pit toilets…it was during those old days, but now…(female, civil servant/farmer, 47 years old, Imo State).
In our community, I can tell you that about 70% of the people have good toilets; it is only about 30% that do not have good toilets. 70% use a water system or closet, if not 80%. So, the other ones, like 10%, use pit toilets, while 5% don’t have toilets; they do open defecation; they go to any nearby bush to defecate” (male, teacher, aged 50 years, Imo State).
The table also shows that only 142 (38.2%) of the deceased had access to pipe-borne water in their houses before their death, while a significant 230 (61.8%) never had access to such an essential facility in their lifetime. This lack of access to a safe and reliable water supply raises serious concerns regarding hygiene, health, and quality of life, especially in communal living areas and among those with poor toilet facilities. This finding also corroborated the IDI data, as a majority of the IDI reported that the deceased had no access to pipe-borne water in their houses before their death. One of the IDI respondents categorically stated:
I can say water is actually a problem for us because boreholes are rare. We only have rivers and wells; even in our river, there is a well beside it. Our water sources are actually from wells and rivers with few boreholes. There is no one person with pipe-borne water in his or her house, not even those that have died (female, student, 21 years old, Ebonyi State).
One of the IDI respondents also noted that “we rarely have such a facility in our community; it is only a few that are very comfortable that can really have pipe-borne water in their houses. In fact, when it comes to the type of water that is running in the house, it’s few. So, pipe-borne water or whatever, we don’t have it at all; it’s only boreholes and streams (natural spring water). These are the major ones; there is no pipe-borne water in this community (male, teacher, aged 50 years, Imo State).
The findings suggest a population that is predominantly living in communal or informal settings, with limited access to private sanitation and clean water. Although a reasonable proportion live in structurally sound housing (bungalows and block houses), sanitation and water supply infrastructure remain inadequate for many. These insights point to the need for targeted interventions in urban planning, housing development, water supply expansion, and sanitation improvements to enhance living conditions and promote public health.
Table 7 shows that the sanitary condition of residences of a majority of 265 (71.2%) of the deceased is clean, while those of 25 (6.7%) of them are very clean. The data, however, show that the sanitary conditions of residences of some deceased, 32 (8.6%) and 50 (13.4%), are waterlogged and filled with dirt, respectively. This partly corroborated the IDI data as an IDI respondent said:
Yes, down here we have good sanitary conditions. I told you that you can hardly hear of adolescent deaths or adult deaths due to diarrhea. Since we keep everywhere neat, that makes us not die prematurely. I only have diarrhea if I eat something that is not good, but when I correct myself, the thing will stop. So not that we don’t suffer from diarrhea, but we hardly die from it. Let me also tell you, we even keep our toilets clean, and we hardly die of diarrhea (female, civil servant/farmer, 47 years old, Imo State).
Another said, “Yes! The sanitary condition here, I can say that about 90% is ok. Let’s say 70% are standard, while sub-standard is like 30%; yes, 30% is not all that conducive” (male, teacher, 50 years old, Imo State).
Conversely, another female respondent had this to say:
Some people are dirty; if you like, bathe a pig, a pig remains a pig. You will see some houses well-built, but the people living there, they mess up everywhere. So, sanitation is not that encouraging here, and this kind of sanitary condition can cause diarrhea and death (female, nurse, 52 years old, Imo State).
The divergence in sanitary conditions of people’s residences could portray the poor sanitary attitudes of some people towards their homes, largely orchestrated by ignorance, illiteracy, poor upbringing, belief system, lack of exposure, and nature of occupation.
Test of hypothesis
Hypothesis 1
There is a significant relationship between the provision of basic social amenities and deaths by diarrhea in South-East Nigeria.
The multiple regression analysis in Table 8 demonstrates that access to pipe-borne water is significantly associated with lower diarrhea mortality (β = -0.42, p < 0.001). Similarly, having a water system toilet compared to open defecation is associated with reduced diarrhea mortality (β = -0.36, p = 0.001). Environmental conditions categorized as “filled with dirt” were associated with increased diarrhea mortality (β = 0.34, p = 0.035). The overall model explains 39% of the variance in diarrhea mortality (R2 = 0.39, p < 0.001).

Table 8. Multiple regression analysis of social amenities and diarrhea mortality.
Discussion
The study was a perception on the effect of the provision of basic social amenities and deaths through diarrhea in South-East Nigeria with the objective of examining the relationship between the provision of basic social amenities and death by diarrhea in the study area. The findings strongly support the relationship between access to social amenities—particularly clean water infrastructure—and diarrhea mortality. Access to pipe-borne water emerged as the strongest protective factor (β = -0.42, p < 0.001), followed by having a water system toilet (β = -0.36, p = 0.001). This corroborated the qualitative data. These results confirm previous research highlighting the importance of WASH interventions in reducing diarrheal disease burden (2, 3, 8, 9).
The fact that housing type and environment type were not significantly associated with diarrhea mortality suggests that specific infrastructure elements (water access, toilet facilities) may be more important than general living conditions. This has important implications for prioritizing public health investments in resource-limited settings.
Conclusion
The study looked at the effect of basic social amenities and deaths by diarrhea in South-East Nigeria and showed a significant relationship between basic social amenities and mortality by such communicable diseases as diarrhea in the area of study. Access to clean water and improved sanitation facilities are strongly associated with reduced diarrhea mortality. This underscores the importance of addressing social determinants of health alongside biomedical interventions in efforts to reduce deaths occurring as a result of communicable diseases. Integrated approaches that combine intensive awareness creation/education on the prevention of communicable diseases, behavioral interventions, and infrastructure improvements are likely to yield the greatest health benefits in this geopolitical zone.
Limitations
This study has some limitations. The cross-sectional design limits causal inference, and the bias in recalling the information about the deceased may affect the accuracy of such information about the deceased. Future research should employ longitudinal designs and consider additional socioeconomic factors that may influence communicable disease mortality. Besides, bias in the creation of population categories may badly affect sample size and subsequently, generalization, as there could be some other useful relevant population categories that may have escaped the mind of the researchers at the time of planning the study; and this, further, makes the future consideration of longitudinal surveys desirable.
Recommendations
These findings suggest several policy implications:
1. Infrastructure investments should prioritize clean water access and improved sanitation facilities, even in areas where general housing conditions are adequate. Point-of-use water treatment solutions may offer interim benefits while larger infrastructure projects are developed.
2. Workplace health programs targeting food safety and hygiene practices are needed, particularly in public service and business/trading sectors. These should include safe food handling practices and access to clean water and sanitation facilities in workplaces.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author.
Ethics statement
The study was conducted in compliance with ethical principles. Ethical approval for this study was obtained from the Directorate of Research and Publications, Abia State University, Uturu.
Author contributions
OI: Conceptualization, Writing – original draft, Data curation, Formal analysis, Interpretation, Qualitative analysis, Writing – review & editing, Approval of final manuscript. JUI: Data curation, Qualitative analysis, Writing – review & editing, Approval of final manuscript.
Funding
This work was part of the study funded by the Tertiary Education Trust Fund (TETFund) in Nigeria (Grant number: TETFund/IBR/ABSU/2024/006).
Competing Interests
The authors declare no competing interests.
Acknowledgments
We acknowledge the Tertiary Education Trust Fund (TETFund) Nigeria for funding the execution of this study. Again, we extend our appreciation to the research assistants for playing a key role in the data collection.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Das JK, Lassi ZS, Salam RA. Effect of community based interventions on childhood diarrhea and pneumonia: uptake of treatment modalities and impact on mortality. BMC Public Health. (2013) 13(Suppl 3):S29. doi: 10.1186/1471-2458-13S3-S29
2. World Health Organization.Diarrhoea disease. WHO (2024). Available online at: www.who.int/news-room/fat-sheets/detail/diarrhoea-disease (Accessed August 29, 2025).
3. Nwokoro UU, Ugwa O, Onwuliri CD, Obi IF, Ngozi M, Agunwa C. Water, sanitation, and hygiene risk factors associated with diarrhea, morbidity in a rural community of Enugu, South-East Nigeria. Pan Afr Med J. (2020) 2(37):115. doi: 10.11604/pamj.2020.37.115.17735
4. Azanaw J, Malede A, Yalew HF, Worede EA. Determinants of diarrhoeal diseases among under-five children in Africa (2013-2023): a comprehensive systematic review highlighting geographic variances and environmental factors. BMC Public Health. (2024) 24:2399. doi: 10.1186/s12889-024-19962-0
5. Worede EA, Malede A, Feleke H, Abere G, Demeke EA, Azanaw J. Prevalence of diarrheal diseases and associated factors among under five children in Africa: a meta-analysis. PLoS One. (2025) 20(7):e0326501. doi: 10.1371/journal.pone.032650
6. Workie GY, Akalu TY, Baraki AG. Environmental factors affecting childhood diarrheal disease among under-five children in Jamma District South Wetto Zone, Northeast Ethiopea. BMC Infect Dis. (2019) 19:804. doi: 10.1186/s12879-019-4445-x
7. Nemeth V, Pfieghaar N. Diarrhoea. StatPearls (2022). Available online at: https://www.ncbi.nlm.nih.gov (Accessed August 29, 2025).
8. Wolf J, Prüss-Ustün A, Cumming O, Bartram J, Boujour S, Cairncross S, et al. Assessing the impact of drinking water and sanitation on diarrhoeal disease in low- and middle-income settings: systematic review and meta-regression. Trop Med Int Health. (2014) 19(8):928–42.
9. Merid MW, Alem AZ, Chilot D, Belay DG, Kibret AA, Asratie MH, et al. Impact of access to improved water and sanitation on diarrhea reduction among rural under-five children in low and middle-income countries: a propensity score matched analysis. Trop Med Health. (2023) 51:36. doi: 10.1186/s41182-023-00525-9
10. Mohamed ESE. Contribution of water, sanitation, hygiene and basic education to reduce under-five mortality in Sudan. J Water Sanit Hyg Dev. (2024) 14(8):616–32. doi: 10.2166/washdev.2024.215
11. Rebecca AO. Effect of basic amenities on socio-economic development of rural areas in Benue State. Wukari Int Stud J. (2024) 8(1):128–42.
12. National Population Commission (NPC) (Nigeria) & ICF.Nigeria Demographic and Health Survey 2018. Abuja, Nigeria and Rockville, Maryland, USA: NPC and ICF (2019).
13. World Bank Group.Curbing Mortality Among Slum Dwellers: The Health Status of the Urban Poor in Kenya. African Population and Health Research Center (2015). Available online at: www.Aphrc.org/…/policy_brife_curbing-mortality-in-Nairobis-Slums-Aug-2015…
14. World Health Organization.Water for Health-Taking Charge. WHO World Water Day Report (2001). Available online at: www.who.int/water_sanitation_health/takingcharge.html
15. National Population Commission (NPC) & ICF International.Nigeria Demographic and Health Survey, 2013. Abuja, Nigeria and Rockvile Maryland USA: NPC & ICF International (2014).
16. Van Lerberghe W, De Brouwere V. Of blind alleys and things that have worked: history’s lessons on reducing maternal mortality. In: De Brouwere V, Van Lerberghe W editors. Safe Motherhood Strategies: A Recent Review of the Evidence. Antwerp: ITG Press (2001). p. 7–33.
18. Haralambos M, Holborn M. Socioogy: Themes and Perspectives. London: HarperCollins Publishers Limited (2008).
19. Tomasini F. What and when is death? In: Tomasini F editor. Remembering and Disremembering the Dead. Palgrave Historical Studies in the Criminal Corpse and its Afterlife. London: Palgrave Macmillian (2017). doi: 10.1057/978-1-137-53828-4_2
20. Leming MR, Dickinson GE. Understanding Dying, Death and Bereavement. 5th ed. Fort Wort, TX: Harcourt (2002).
22. Fabis A, Kilimczuk A. Death and dying, theories of. In: Turner BS, Kivisto P, Outhwaite W, Chang K-S, Epstein C, Ryan JM , editors. The Wiley-Blackwell Enceclopedia of Social Theory. Hoboken, NJ: Wiley (2017). doi: 10.1002/9781118430873.est0084
23. Walter T. Death and dying, sociology of. In: Wright JD , editor. International Encyclopedia of the Social & Behavioral Sciences. 2nd ed. Oxford, UK: Elsevier (2015). p. 865–869. Available online at: https://researchportal.bath.ac.uk (Accessed August 29, 2025).
24. Baloyi L. The African Conception of Death: A Cultural Implication. (2014). Available online at: https://www.scholarwork.gvsu.edu (Accessed August 29, 2025).
25. Nnoruga JN. The Concept of Death in the Changing World of African Worldview. (2024). Available online at: https://www.acjol.org (Accessed August 29, 2025).
26. Cleveland Clinic.Diarrhoea: Causes, Symptoms and Treatment. Cleveland Clinic (2025). Available online at: https://my.clevelandclinic.org (Accessed August 29, 2025).
27. Atimati AO, Eki-Udoko FE. Diarrhea prevalence, characteristics and outcome among children admitted into the emergency ward of a tertiary hospital in Southern Nigeria. Ann Clin Biomed Res. (2022) 3(218). doi: 10.4081/acbr.2022.218
28. Hughes M, Koehler CJ, Zanden JWV. Sociology the Core. 6th ed. New York: McGraw-Hill companies, Inc (2002).
29. Fasan R. Will there be peace in our time? The National Scholar. A. Publication of the Academic Staff Union of Universities (ASUU) (2011) 8:36.
30. Caldwell JC, Bruce KC, Pat C, Peter FM, Thomas S. Demographic Transition Theory Dordrecht. The Netherland: Springer (2006).
31. National Population Commission & ICF Macro.Nigerian Demographic and Health Survey 2008. Calverton Maryland: NPC (2009).
32. Goliber JT. Population and Reproductive Health in Sub-Saharan Africa. Vol. 52, No. 4 of Population Bulletin. Washington DC: Population Reference Bureau (1997).
33. Adetunji J, Bos ER. Levels and trends in mortality in sub-Saharan Africa. An overview. 2nd ed. In: Jamison DT, Feachem RG, Makgoba MW, et al. editors. Disease and Mortality in Sub-Saharan Africa. Washington DC: World Bank (2006).
34. Nwoye CMA. Igbo cultural and religious worldview: an insider’s perspective. Int J Sociol Anthropol. (2011) 3(9):304–17.
© The Author(s). 2025 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.