Introduction
Deep Brain Stimulation (DBS) is a high frequency, pulsatile, monopolar/bipolar electrical stimulation through a stereotactically placed electrode into a target nucleus which can be activated and deactivated with an external magnet. Its exact physiology is unknown, but higher frequencies mimic cellular ablation and not stimulation.
Indications for DBS
• Parkinson’s disease
– STN/Gpi
• Primary generalized dystonia
– Gpi
• Essential tremor
– Vim
• Obsessive compulsive disorder
– ALIC/BNST
• Tourette’s syndrome
– Gpi
• Drug-resistant major depression
– ALIC
• Drug-resistant epilepsy
– ANT/CM
• Minimally conscious state
• Alcohol or other addictions
• Post-traumatic stress disorder
Patient selection criteria for Parkinson’s disease DBS
• Inclusion criteria
– Diagnosis of PD
– Response to levodopa
– UPDRS
– Dopa challenge testing
– Dyskinesias and motor fluctuations
• Exclusion criteria
– Severe brain atrophy or Ischaemia
– Impulse control disorders
– Major depression
– Dementia
– Advanced age
– Anesthetic risk/bleeding risk
The patient and family members should be educated about having realistic expectations since they may fail to appreciate any improvement if expectations from surgery are too high.
Surgery process flow

Planning MRI is done a day or two prior to the date of surgery. It is ideally done under general anesthesia in order to minimize movement artifacts in the MRI and thereby improve accuracy of identifying the target (Figure 1).
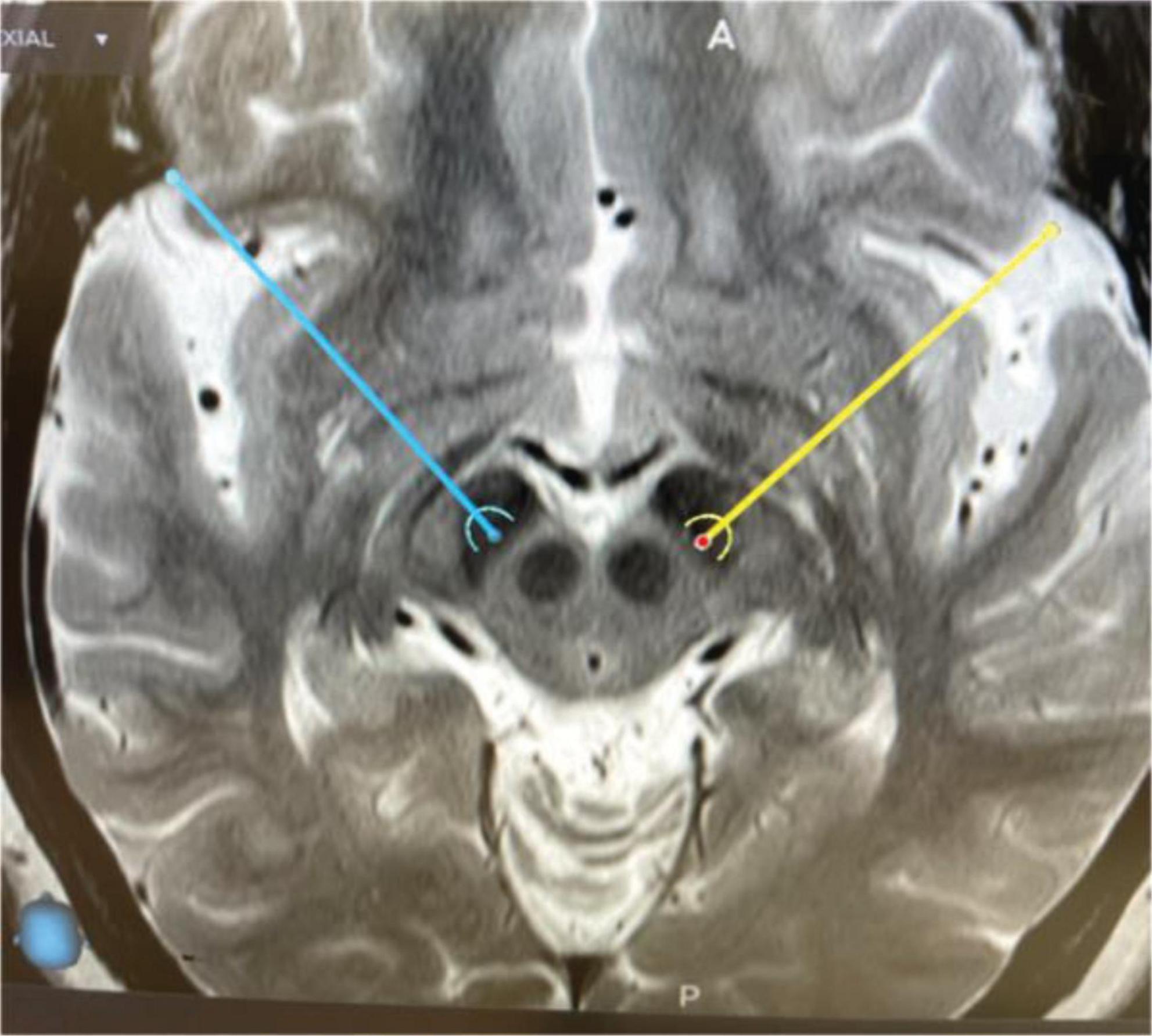
Figure 1. Axial T2W MRI image showing the planned target into both the subthalamic nuclei.
Typical stereotactic coordinates for common DBS targets

On the day of surgery, the stereotactic frame’s base ring is applied under local anesthesia and the patient undergoes CT with the indicator box on. This CT image is fused with the previously done MRI and the stereotactic co-ordinates are calculated.
In the OT, the frame is assembled, burrhole is made on one side (usually the more affected side) and the micro electrode recorder’s Ben-Gun array is set up and as many MER tracts are studied as required. Once satisfactory MER recordings of the STN are obtained, macrostimulation is done to get an idea of the best clinical effect and side effect profile. Based on this information the final DBS electrode is implanted and secured with an electrode securing device that also closed the burrhole site. The same process is repeated on the opposite side and thereafter a repeat CT is done to confirm the position of the electrode.
Following this, the IPG is implanted under general anesthesia using extension cables. I prefer a subcutaneous pocket in the left infraclavicular region for my IPG’s.
Post-operative course

Usual settings at the initiation of programming
• Select the contact
• Usually monopolar
• Freq 130 Hz
• PW 60
• Amplitude is the one variable that is usually increased gradually as per the symptomatic response.
Complications of surgery
• Life threatening <0.5%
– Major bleeding
– Risk to life
• Stimulation related 3–10%- usually reversible with change of the contact or programming settings.
• Infection 2–3%- sometimes necessitates implant exit.